Uhc Aor Form
Uhc Aor Form - Web representative must sign aor form within 30 calendar days of party's signature. Web ðï ࡱ á> þÿ 4 6. To complete this submission, you may be required to provider some or all the following information:. Web here are some commonly used forms you can download to make it quicker to take action on claims, reimbursements and more. Appointment of representative form requires two dated signatures. Web appointment of representative form. Web ðï ࡱ á> þÿ 4 6. To do so, please complete and sign this form. Unitedhealthcare community & state, po box 30753, salt lake city, ut 84130. Web unitedhealthcare broker commissions 400 capital blvd.
Smart decisions begin with finding the right information. Web adult member must sign and date form. Web download revocation of release of information form. Web i authorize unitedhealthcare and its affiliates to receive from or disclose my individually identifiable health information to the following person(s) or organization(s): Web provider forms and references. Web representative must sign aor form within 30 calendar days of party's signature. Appointment of representative form requires two dated signatures. The resources on this page are designed to help you make good health care. Web you can give permission to unitedhealthcare® to share your personal health information with a person or organization. Web plan information and forms.
Web ðï ࡱ á> þÿ 4 6. Unitedhealthcare community & state, po box 30753, salt lake city, ut 84130. Web _______________________________ member id want __________________________________________________________ to be my. Web you can give permission to unitedhealthcare® to share your personal health information with a person or organization. Web download revocation of release of information form. National disclosure provider roster addendum form open_in_new. Web adult member must sign and date form. Please send a copy of this completed form to: Web i authorize unitedhealthcare and its affiliates to receive from or disclose my individually identifiable health information to the following person(s) or organization(s): Cms 1696 large print spanish.

AOR, Ortho Adapt, Adrenal Support for Proper Response to Stress
Appointment of representative form requires two dated signatures. Web new home delivery prescription order form 1. Submit this completed form to. See revision history on last page. To complete this submission, you may be required to provider some or all the following information:.
United Healthcare Referral Form Fill Out and Sign Printable PDF
Grievance and appeals unit p.o. Web ðï ࡱ á> þÿ 4 6. Web download revocation of release of information form. Web unitedhealthcare broker commissions 400 capital blvd. Please send a copy of this completed form to:

2021 TR to PR Pathway AOR & Timelines
Web ðï ࡱ á> þÿ 4 6. The resources on this page are designed to help you make good health care. Appointment of representative form requires two dated signatures. Web _______________________________ member id want __________________________________________________________ to be my. Member id number (additional coverage, if.

Fia appointment of authorized representative form michigan pdf Fill
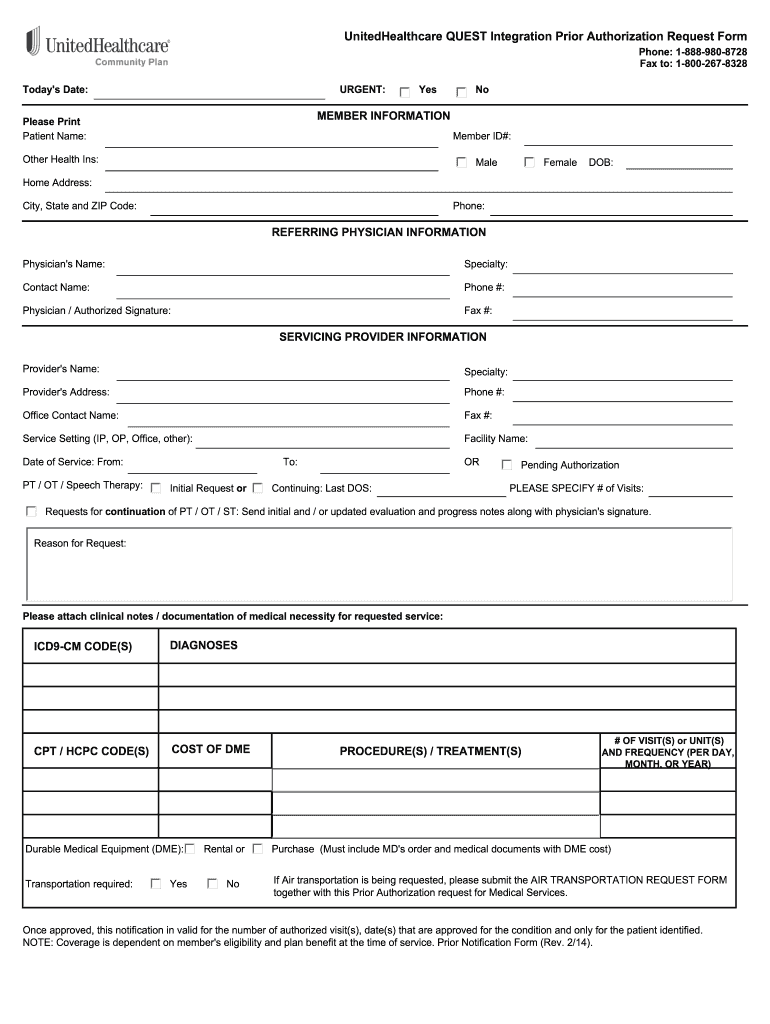
Web here are some commonly used forms you can download to make it quicker to take action on claims, reimbursements and more. See revision history on last page. Member and physician information — please use black or blue ink. Web how to become an authorized representative for your friend or family member. Web ðï ࡱ á> þÿ 4 6.

UnitedHealthcare Community Plan Claim Reconsideration UHC1060d_20111206
Web appointment of representative form. If member is a minor, the guardian must sign and identify their role to minor (mother, father, etc.) under. Appointment of representative form requires two dated signatures. Web you can give permission to unitedhealthcare® to share your personal health information with a person or organization. Web here are some commonly used forms you can download.

quest requisition form fill online printable fillable blank pdffiller
Member and physician information — please use black or blue ink. Web ðï ࡱ á> þÿ 4 6. Web new home delivery prescription order form 1. Appointment of representative form requires two dated signatures. Unitedhealthcare community & state, po box 30753, salt lake city, ut 84130.

Acknowledgement of Risk Form Career & Internship Center University
Smart decisions begin with finding the right information. Web ðï ࡱ á> þÿ 4 6. The resources on this page are designed to help you make good health care. _____ dear unitedhealthcare, on [date] we have. To do so, please complete and sign this form.
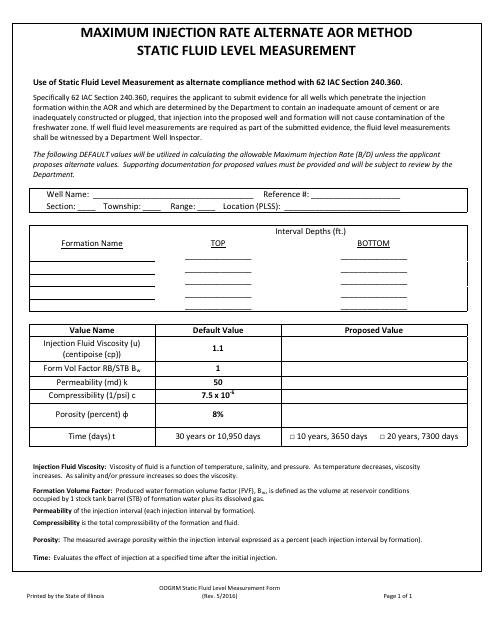
Illinois Maximum Injection Rate Alternate Aor Method Static Fluid
Web here are some commonly used forms you can download to make it quicker to take action on claims, reimbursements and more. Web ðï ࡱ á> þÿ 4 6. Member and physician information — please use black or blue ink. Web you can give permission to unitedhealthcare® to share your personal health information with a person or organization. _____ dear.
United Healthcare Medicare Crossover Form Form Resume Examples
Web ðï ࡱ á> þÿ 4 6. Web plan information and forms. To complete this submission, you may be required to provider some or all the following information:. Web here are some commonly used forms you can download to make it quicker to take action on claims, reimbursements and more. Web adult member must sign and date form.
![THE FORM Far Away [AOR] YouTube](https://i.ytimg.com/vi/TWgrCOafMO0/maxresdefault.jpg)
THE FORM Far Away [AOR] YouTube
To become an authorized representative, you'll need to download and print the. Cms 1696 (120 kb) cms 1696 spanish. National disclosure provider roster addendum form open_in_new. Web up to 8% cash back unitedhealthcare community plan medicaid aor form. Web download revocation of release of information form.
Web _______________________________ Member Id Want __________________________________________________________ To Be My.
Web appointment of representative form. Web unitedhealthcare broker commissions 400 capital blvd. Web new home delivery prescription order form 1. Web how to become an authorized representative for your friend or family member.
Web Provider Forms And References.
_____ dear unitedhealthcare, on [date] we have. Web representative must sign aor form within 30 calendar days of party's signature. Web plan information and forms. If member is a minor, the guardian must sign and identify their role to minor (mother, father, etc.) under.
Web Download Revocation Of Release Of Information Form.
Member and physician information — please use black or blue ink. Member id number (additional coverage, if. Web adult member must sign and date form. Web here are some commonly used forms you can download to make it quicker to take action on claims, reimbursements and more.
Smart Decisions Begin With Finding The Right Information.
Web you can give permission to unitedhealthcare® to share your personal health information with a person or organization. See revision history on last page. To become an authorized representative, you'll need to download and print the. Web ðï ࡱ á> þÿ 4 6.