Synagis Prior Authorization Form
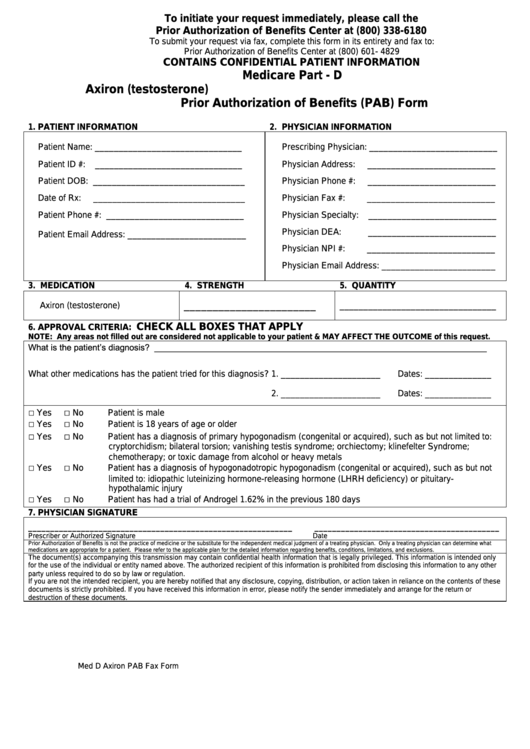
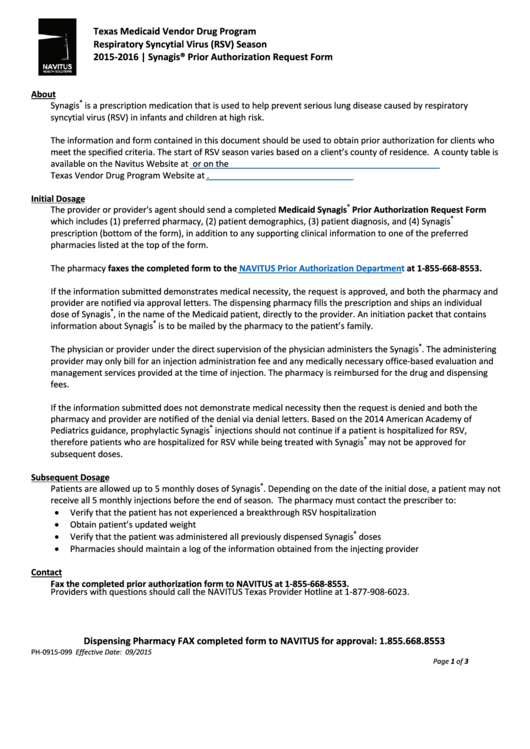
Synagis Prior Authorization Form - Billing provider information (pharmacy, physician, or. Web prior approval request. Web synagis prior authorization please fax this completed form to: This is an optum prior authorization criteria specific form to enroll or prescribe rsv and. Billing provider npi section ii —. Prior authorization drug attachment for synagis. The synagis® prior authorization (pa) request form for nc medicaid direct beneficiaries is found on the nctracks pharmacy services page. Calculated dosage of synagis (15 milligrams per kilogram of body weight) 14. Web synagis® prior authorization form for rsv season: Web this patient’s benefit plan requires prior authorization for certain medications in order for the drug to be covered.
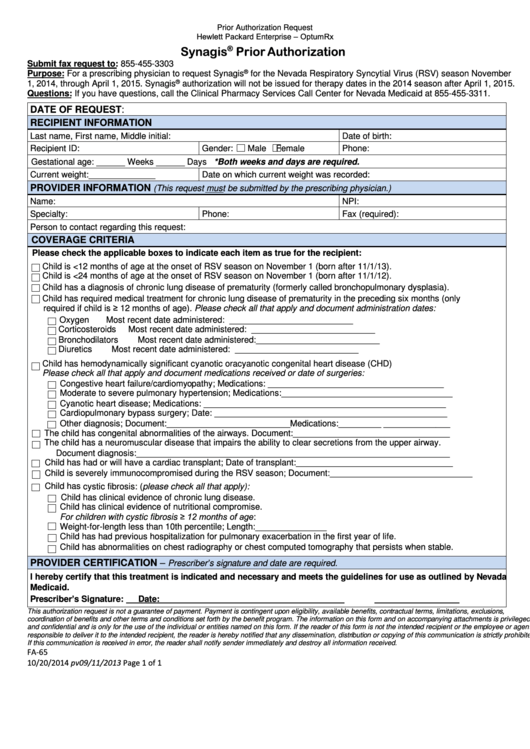
Prescribers are required to retain. Providers may call the drug authorization and policy. Web this patient’s benefit plan requires prior authorization for certain medications in order for the drug to be covered. Billing provider npi section ii —. Web effective july 29, 2022, prior authorization requests for synagis will be considered for approval of 2 doses at least 30 days apart. Web synagis® prior authorization form for rsv season: To make an appropriate determination, providing the most. The synagis® prior authorization (pa) request form for nc medicaid direct beneficiaries is found on the nctracks pharmacy services page. Web universal synagis authorization form *fax the completed form or call the plan with the requested information. Calculated dosage of synagis (15 milligrams per kilogram of body weight) 14.
This is an optum prior authorization criteria specific form to enroll or prescribe rsv and. Web effective july 29, 2022, prior authorization requests for synagis will be considered for approval of 2 doses at least 30 days apart. Providers may call the drug authorization and policy. Web universal synagis authorization form *fax the completed form or call the plan with the requested information. Web all requests for synagis (palivizumab) require a prior authorization and will be screened for medical necessity and appropriateness using the criteria listed below. Web synagis® prior authorization form for rsv season: Web synagis prior authorization please fax this completed form to: Calculated dosage of synagis (15 milligrams per kilogram of body weight) 14. Web up to 8% cash back synagis referral form optum specialty rsv referral form for synagis. To make an appropriate determination, providing the most.

Fill Free fillable Sunshine Health PDF forms
Web universal synagis authorization form *fax the completed form or call the plan with the requested information. Prescribers are required to retain. Web all requests for synagis (palivizumab) require a prior authorization and will be screened for medical necessity and appropriateness using the criteria listed below. To make an appropriate determination, providing the most. Web synagis prior authorization please fax.
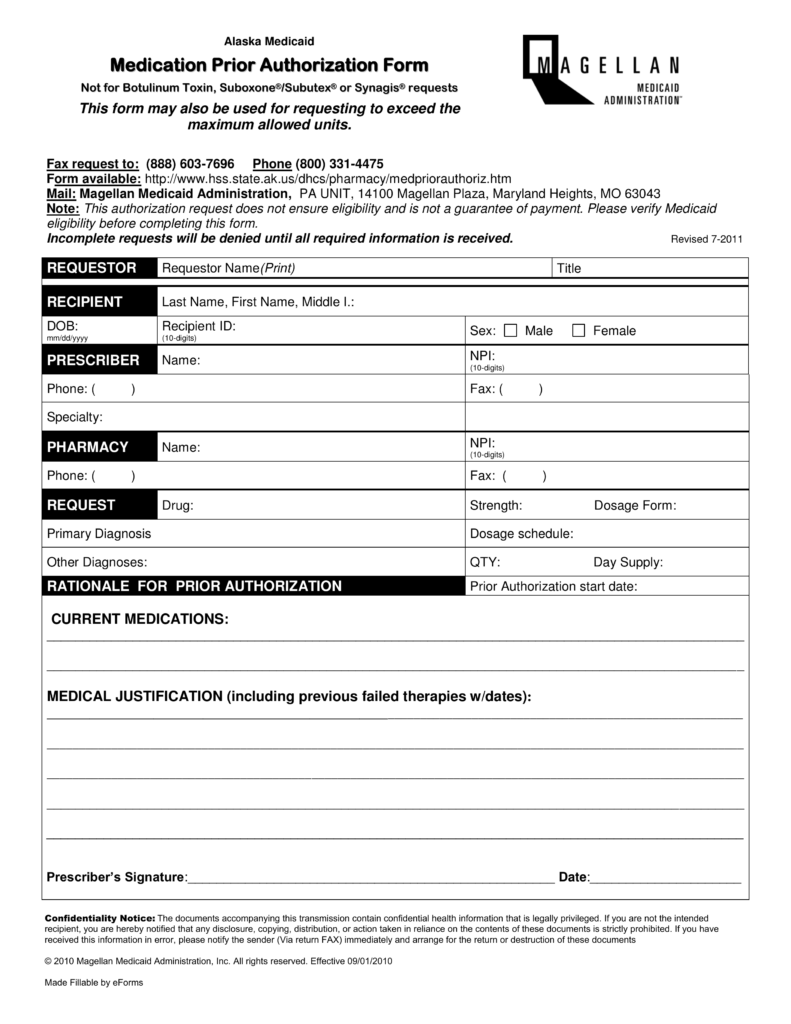
Free Alaska Medicaid Prior (Rx) Authorization Form PDF eForms
Providers may call the drug authorization and policy. Web prior approval request. Prescribers are required to retain. Web effective july 29, 2022, prior authorization requests for synagis will be considered for approval of 2 doses at least 30 days apart. Prescriber address (street, city, state zip+4) 7.
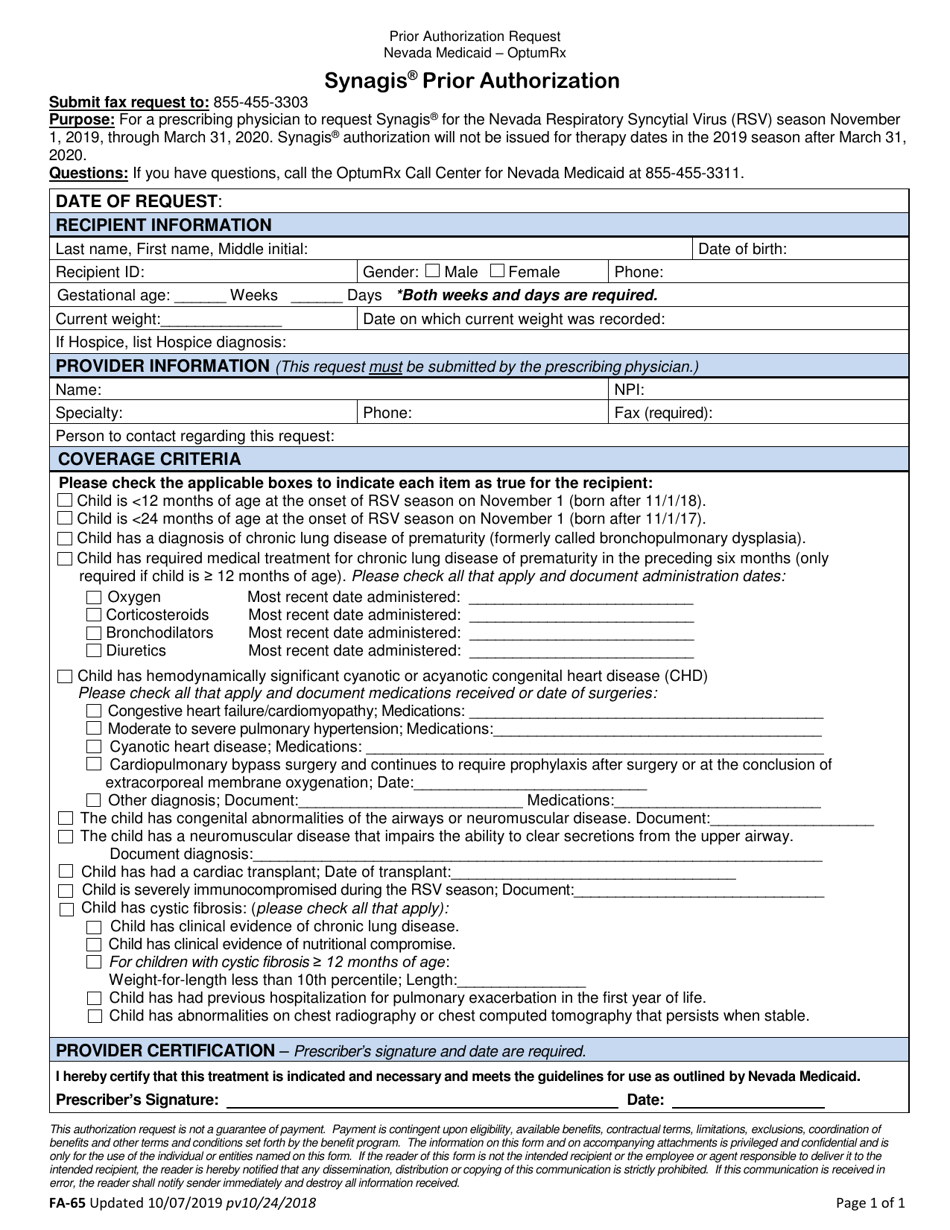
Form FA65 Download Fillable PDF or Fill Online Synagis Prior
Web all requests for synagis (palivizumab) require a prior authorization and will be screened for medical necessity and appropriateness using the criteria listed below. Web prior approval request. Billing provider npi section ii —. Web up to 8% cash back synagis referral form optum specialty rsv referral form for synagis. Web synagis prior authorization please fax this completed form to:
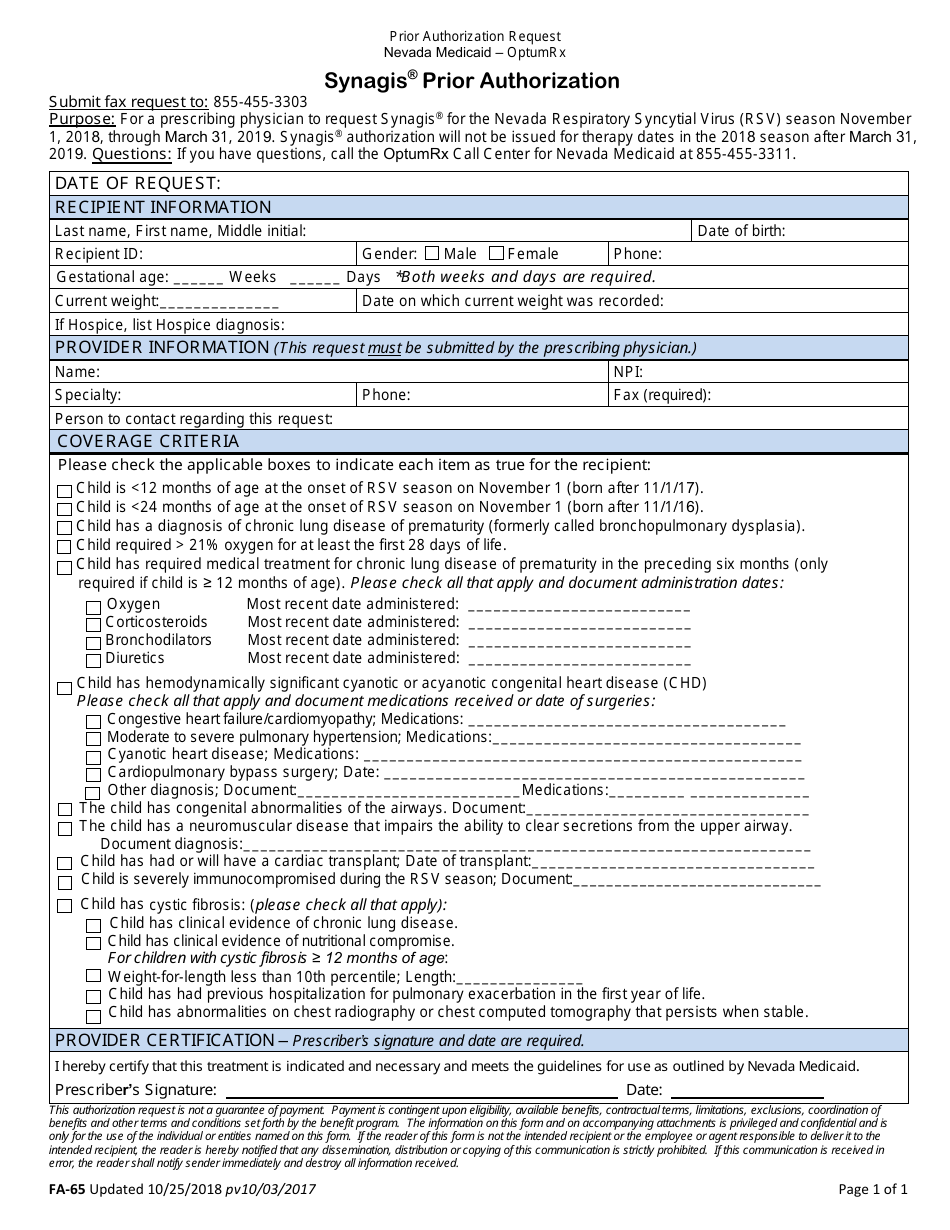
Form FA65 Download Fillable PDF or Fill Online Synagis Prior
This is an optum prior authorization criteria specific form to enroll or prescribe rsv and. If necessary, an additional 2. The synagis® prior authorization (pa) request form for nc medicaid direct beneficiaries is found on the nctracks pharmacy services page. Prescribers are required to retain. Prescriber address (street, city, state zip+4) 7.
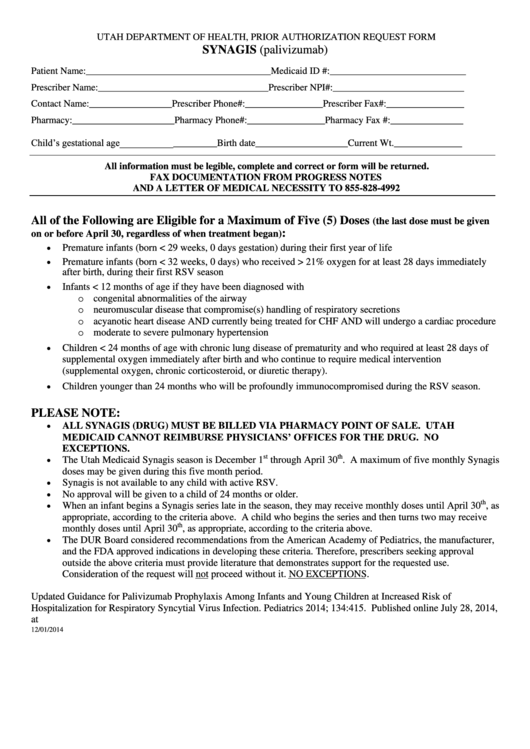
Prior Authorization Request Form (Synagis) Utah Department Of Health
Web all requests for synagis (palivizumab) require a prior authorization and will be screened for medical necessity and appropriateness using the criteria listed below. The synagis® prior authorization (pa) request form for nc medicaid direct beneficiaries is found on the nctracks pharmacy services page. Web this patient’s benefit plan requires prior authorization for certain medications in order for the drug.
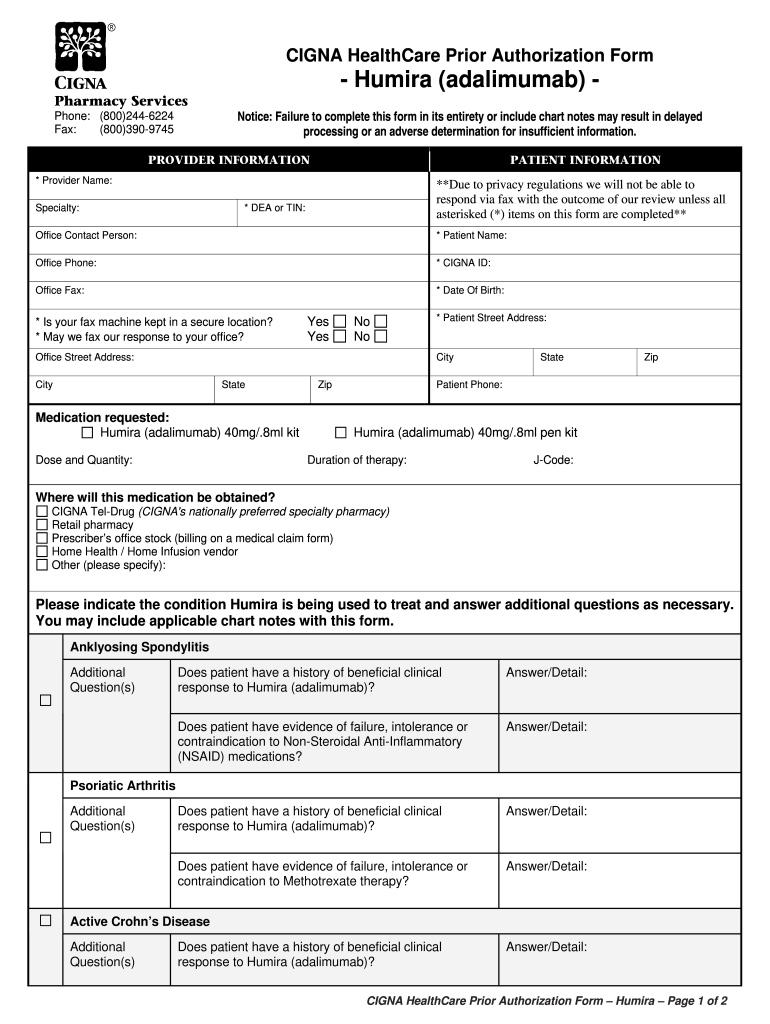
Cigna Biometric Screening Form 2022 Fill Out and Sign Printable PDF
Web synagis prior authorization please fax this completed form to: To make an appropriate determination, providing the most. Web prior approval request. The synagis® prior authorization (pa) request form for nc medicaid direct beneficiaries is found on the nctracks pharmacy services page. Web effective july 29, 2022, prior authorization requests for synagis will be considered for approval of 2 doses.
22 Medicare Prior Authorization Form Templates free to download in PDF
Web all requests for synagis (palivizumab) require a prior authorization and will be screened for medical necessity and appropriateness using the criteria listed below. Calculated dosage of synagis (15 milligrams per kilogram of body weight) 14. All requested data must be. Prior authorization drug attachment for synagis. The synagis® prior authorization (pa) request form for nc medicaid direct beneficiaries is.
Top Navitus Prior Authorization Form Templates free to download in PDF
Billing provider information (pharmacy, physician, or. Web prior approval request. Web up to 8% cash back synagis referral form optum specialty rsv referral form for synagis. Prescriber address (street, city, state zip+4) 7. Web synagis prior authorization please fax this completed form to:
Fillable Fa65 Synagis Prior Authorization Form printable pdf download
Prior authorization drug attachment for synagis. Web synagis® (palivizumab) prior authorization request form beneficiary information name: Web all requests for synagis (palivizumab) require a prior authorization and will be screened for medical necessity and appropriateness using the criteria listed below. Web this patient’s benefit plan requires prior authorization for certain medications in order for the drug to be covered. All.
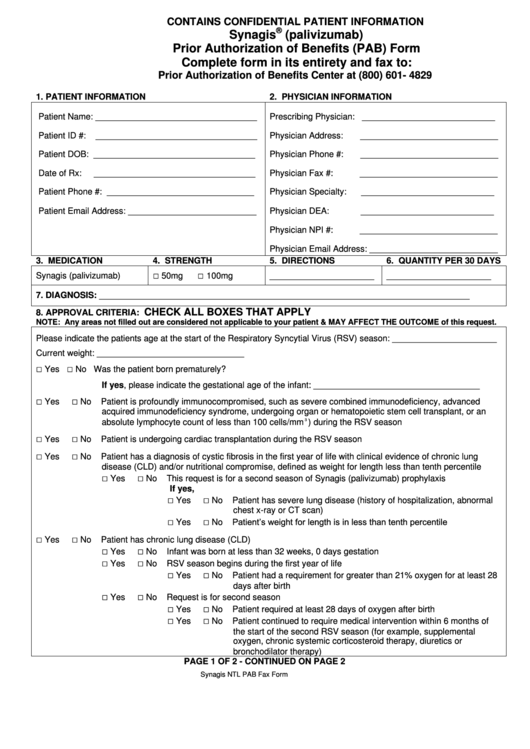
Synagis (Palivizumab) Prior Authorization Of Benefits (Pab) Form
Prior authorization drug attachment for synagis. Web synagis prior authorization please fax this completed form to: Prescriber address (street, city, state zip+4) 7. Calculated dosage of synagis (15 milligrams per kilogram of body weight) 14. All requested data must be.
Prior Authorization Drug Attachment For Synagis.
Web prior approval request. To make an appropriate determination, providing the most. Billing provider information (pharmacy, physician, or. The synagis® prior authorization (pa) request form for nc medicaid direct beneficiaries is found on the nctracks pharmacy services page.
Billing Provider Npi Section Ii —.
This is an optum prior authorization criteria specific form to enroll or prescribe rsv and. Prescribers are required to retain. Web universal synagis authorization form *fax the completed form or call the plan with the requested information. Web effective july 29, 2022, prior authorization requests for synagis will be considered for approval of 2 doses at least 30 days apart.
All Requested Data Must Be.
Web up to 8% cash back synagis referral form optum specialty rsv referral form for synagis. Web synagis® (palivizumab) prior authorization request form beneficiary information name: Web all requests for synagis (palivizumab) require a prior authorization and will be screened for medical necessity and appropriateness using the criteria listed below. Calculated dosage of synagis (15 milligrams per kilogram of body weight) 14.
Web Synagis Prior Authorization Please Fax This Completed Form To:
Providers may call the drug authorization and policy. If necessary, an additional 2. Web synagis® prior authorization form for rsv season: Prescriber address (street, city, state zip+4) 7.