Psychotropic Medication Consent Form
Psychotropic Medication Consent Form - However, once the emergency has passed, your informed consent is required. Propose goals, treatment plans & methods of therapy. Prescriber will discuss with you the information below: Name of medication date of birth dosage range (please print) i. The aprn may consult with a. Psychotropic medication(s) previously used and outcome: 409.912(16) the agency may not pay for psychotropic. Web psychotropic medication consent form anticonvulsants: Consent to treatment by the aprn. ***ensure informed consent form with.
Propose goals, treatment plans & methods of therapy. Web when consenting to a new psychotropic medication, dfps form 4526, psychotropic medication treatment consent must be completed and signed by the medical consenter. Web uses this form to document informed consent for a new psychotropic medication. Web possible to get your consent. Web psychotropic medication(s) recommendation, dose, dosing instructions: 409.912(16) the agency may not pay for psychotropic. Web consent is required for any medication that is used in the treatment of a psychiatric diagnosis or symptom, whether or not the medication is included in this list. Prescriber will discuss with you the information below: Web psychotropic medication consent form anticonvulsants: Web health medical practitioner and you are verifying that the person continues to consent to treatment with this medication.
Web b below for each medication) a if i am taking this medication to assist me in changing my behavior i have a behavioral support plan to address the specific behaviors this. Psychotropic medication(s) previously used and outcome: Propose goals, treatment plans & methods of therapy. Do not upload in misacwis. 409.912(16) the agency may not pay for psychotropic. Prescriber will discuss with you the information below: ***ensure informed consent form with. Choose from 100+ treatment plan templates, wiley notes, billing codes & more Page 2 is for addi onal medica requests.on page 1 must be sent with any addi onal pages. The completion of this form begins with initial contact with the medical provider and continues as information is collected from parents and youth.
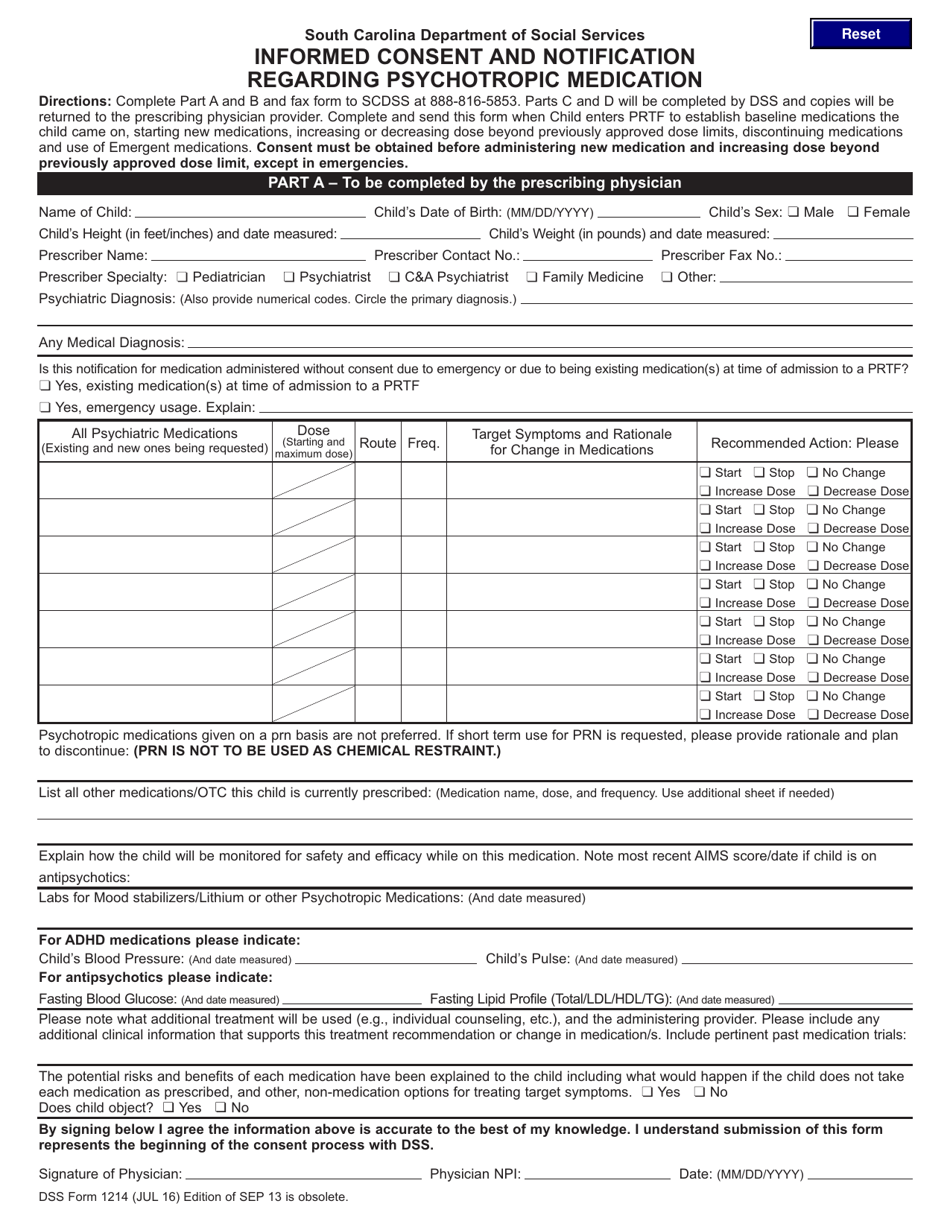
DSS Form 1214 Download Fillable PDF or Fill Online Informed Consent and
Web input on application for psychotropic medication. Web psychotropic medication request form instruc ons: Choose from 100+ treatment plan templates, wiley notes, billing codes & more • prescribing new psychotropic medications. Web consent is required for any medication that is used in the treatment of a psychiatric diagnosis or symptom, whether or not the medication is included in this list.
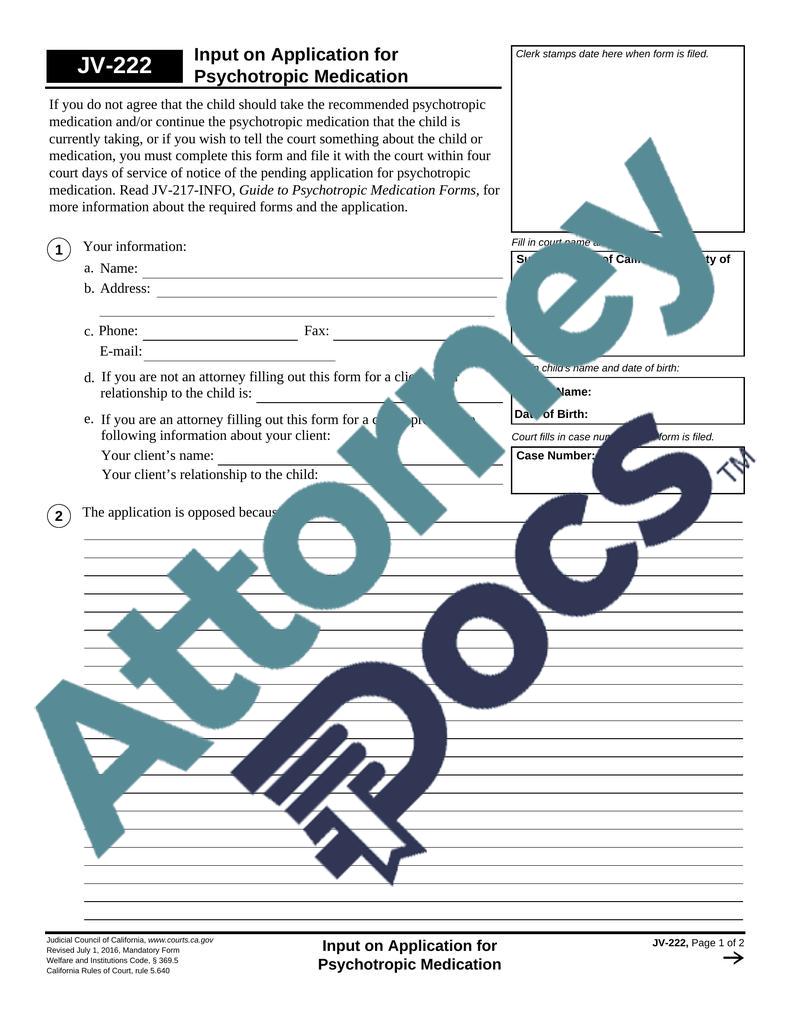
Input on Application for Psychotropic MedicationJuvenile Family Law
Ad what are you waiting for? Complete this form at every medication evaluation appointment. Choose from 100+ treatment plan templates, wiley notes, billing codes & more 409.912(16) the agency may not pay for psychotropic. Choose from 100+ treatment plan templates, wiley notes, billing codes & more
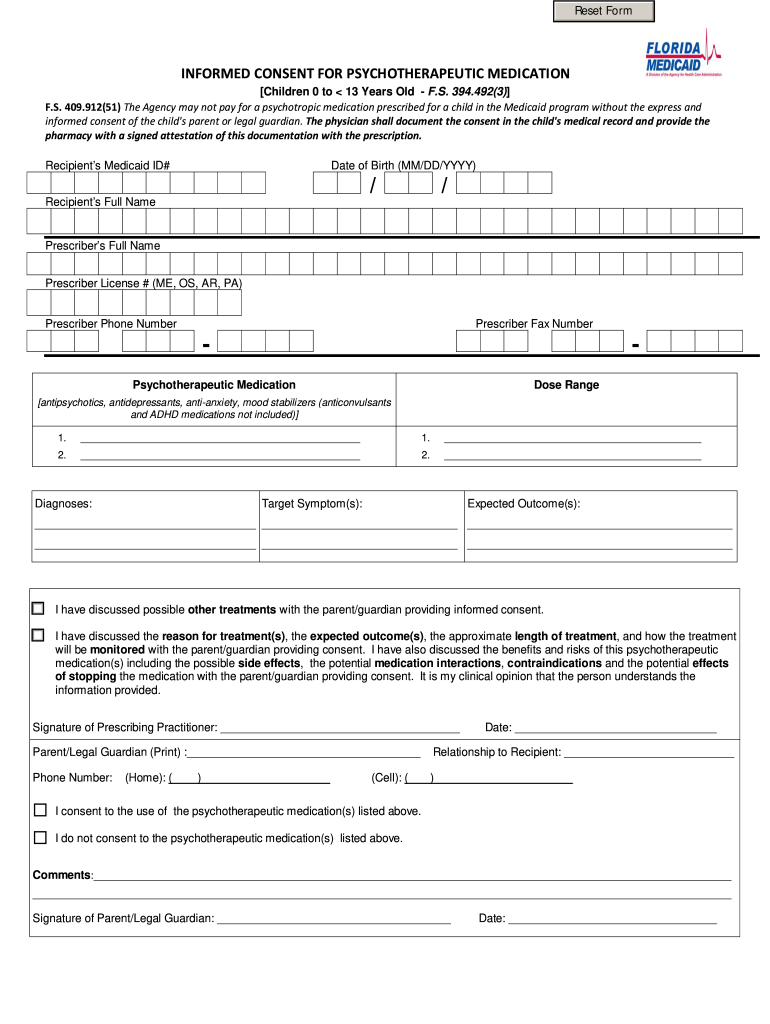
Florida Medicaid Informed Consent Form Fill Out and Sign Printable
409.912(16) the agency may not pay for psychotropic. 409.912(16) the agency may not pay for psychotropic. Web consent for treatment means the student understands and agrees to the following: The aprn may consult with a. Web consent is required for any medication that is used in the treatment of a psychiatric diagnosis or symptom, whether or not the medication is.

(PDF) Psychotropic medication management for youth in state care
Prescriber will discuss with you the information below: Web consent is required for any medication that is used in the treatment of a psychiatric diagnosis or symptom, whether or not the medication is included in this list. Propose goals, treatment plans & methods of therapy. Name of medication date of birth dosage range (please print) i. This form does not.

quick_reference_medication_chart1 Psychiatric medications
Propose goals, treatment plans & methods of therapy. Web possible to get your consent. Web psychotropic medication request form instruc ons: 409.912(51) the agency may not pay for a. Web informed written consent shall be obtained on a form approved by the department, which shall include, at a minimum, the following information:

20192022 Form CA JV217INFO Fill Online, Printable, Fillable, Blank
Ad what are you waiting for? Web uses this form to document informed consent for a new psychotropic medication. Web b below for each medication) a if i am taking this medication to assist me in changing my behavior i have a behavioral support plan to address the specific behaviors this. ***ensure informed consent form with. Web possible to get.
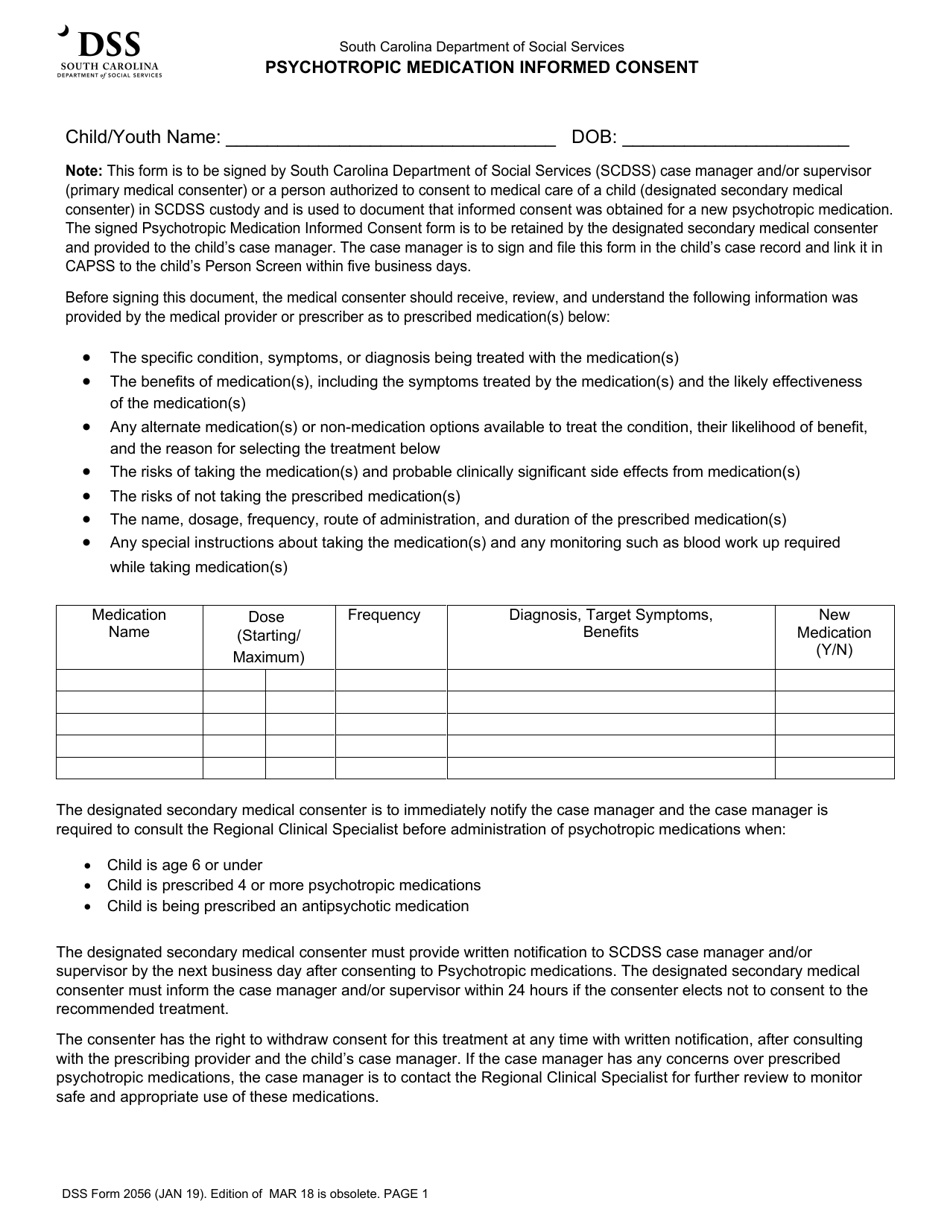
Dss Form 2056 Download Fillable Pdf Or Fill Online Psychotropic
Web health medical practitioner and you are verifying that the person continues to consent to treatment with this medication. Web psychotropic medication(s) recommendation, dose, dosing instructions: Prescriber will discuss with you the information below: 409.912(51) the agency may not pay for a. 409.912(16) the agency may not pay for psychotropic.
Psychotropic Medication Treatment Consent Form(4526)
Page 2 is for addi onal medica requests.on page 1 must be sent with any addi onal pages. Complete this form at every medication evaluation appointment. Healthcare providers may prefer to provide their own documentation regarding information contained in this. Choose from 100+ treatment plan templates, wiley notes, billing codes & more Web the express and informed consent or court.
Medication Consent Form Template Flyer Template
Healthcare providers may prefer to provide their own documentation regarding information contained in this. Web possible to get your consent. Web when consenting to a new psychotropic medication, dfps form 4526, psychotropic medication treatment consent must be completed and signed by the medical consenter. ***ensure informed consent form with. Web consent is required for any medication that is used in.
Informed Consent For Psychiatric Medications printable pdf download
Do not upload in misacwis. Web consent for treatment means the student understands and agrees to the following: Web informed written consent shall be obtained on a form approved by the department, which shall include, at a minimum, the following information: Page 2 is for addi onal medica requests.on page 1 must be sent with any addi onal pages. However,.
Propose Goals, Treatment Plans & Methods Of Therapy.
409.912(16) the agency may not pay for psychotropic. The aprn may consult with a. Typeforms are more engaging, so you get more responses and better data. Propose goals, treatment plans & methods of therapy.
Web Health Medical Practitioner And You Are Verifying That The Person Continues To Consent To Treatment With This Medication.
Choose from 100+ treatment plan templates, wiley notes, billing codes & more Web input on application for psychotropic medication. Ad what are you waiting for? Complete this form at every medication evaluation appointment.
Web Informed Written Consent Shall Be Obtained On A Form Approved By The Department, Which Shall Include, At A Minimum, The Following Information:
409.912(16) the agency may not pay for psychotropic. Web psychotropic medication consent form anticonvulsants: • prescribing new psychotropic medications. Web uses this form to document informed consent for a new psychotropic medication.
Web Psychotropic Medication(S) Recommendation, Dose, Dosing Instructions:
Web consent is required for any medication that is used in the treatment of a psychiatric diagnosis or symptom, whether or not the medication is included in this list. Consent to treatment by the aprn. Name of medication date of birth dosage range (please print) i. ***ensure informed consent form with.