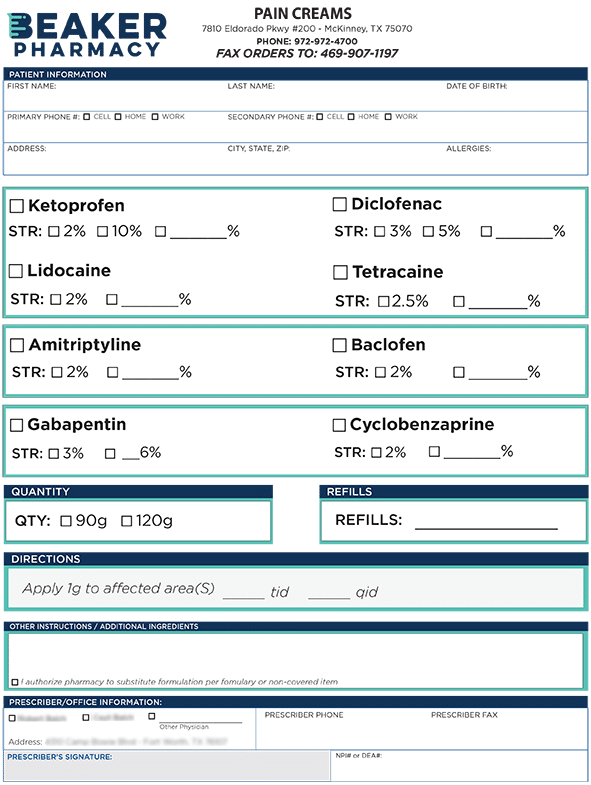
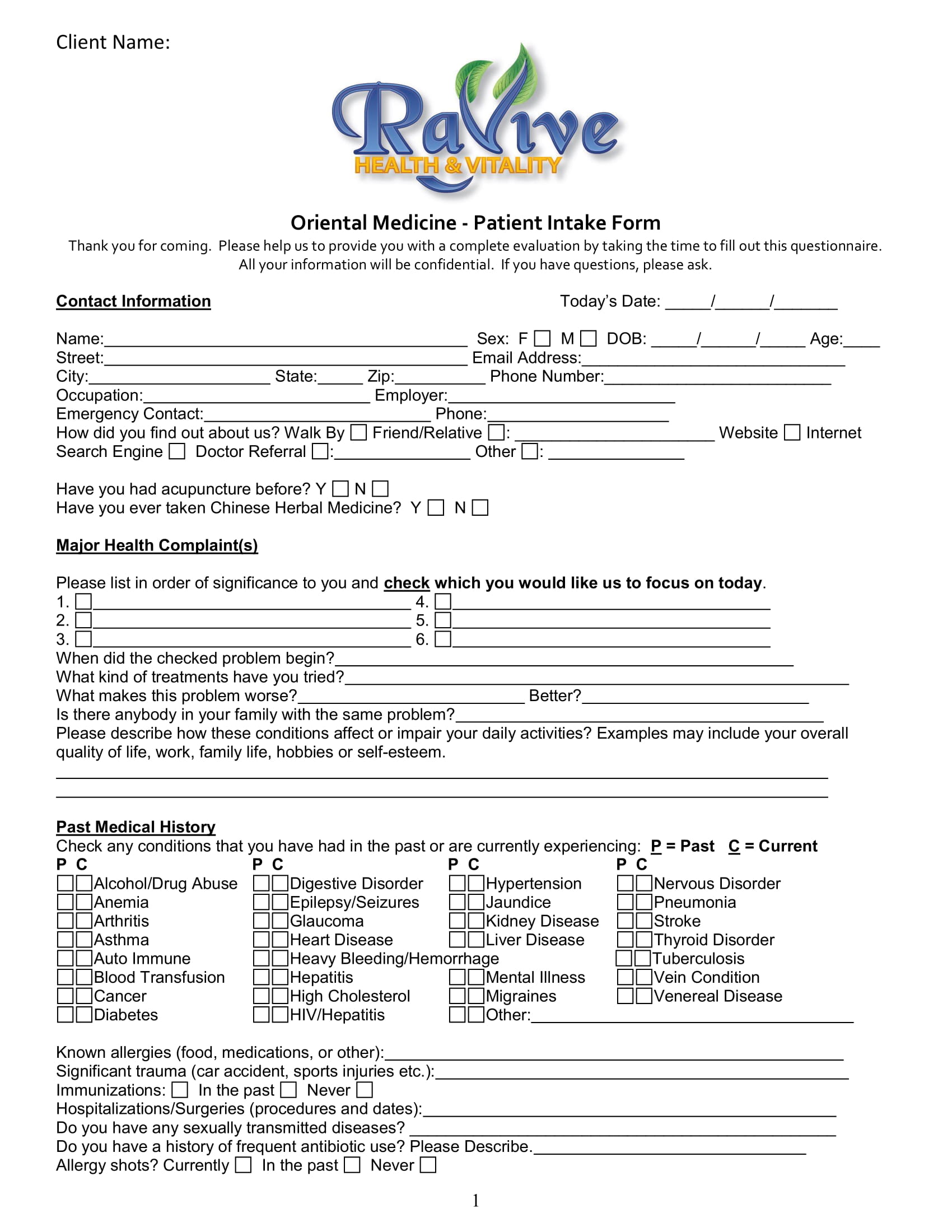
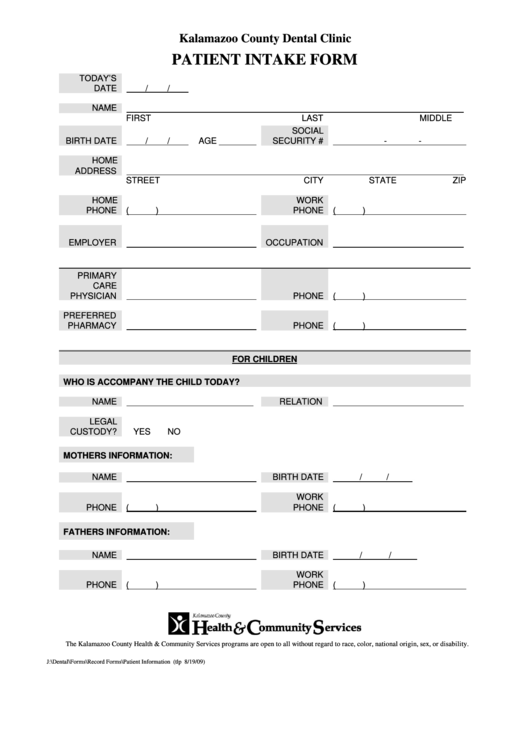
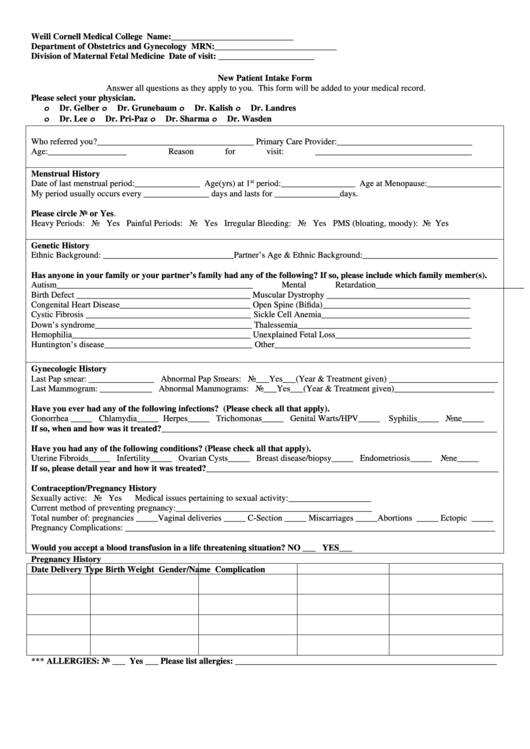
Pharmacy New Patient Intake Form
Pharmacy New Patient Intake Form - Web 1964 new patient intake form name:____date of birth: Simply select get started, fill out the form and submit. Web please enter your date of birth to continue (mm/dd/yyyy) submit Speak with your personal physician about your. Web please consider sending your prescription electronically. Web please consider sending your prescription electronically. Web that's why we offer a quick, simple way to submit your new patient intake form here, online. The form will need information such as patient information and. Web fill out our new patient form to expedite the process and get your prescriptions faster from any of our new york city locations. Try the leading practice management solution for solo and group private practitioners.
Web please enter your date of birth to continue (mm/dd/yyyy) submit Web that's why we offer a quick, simple way to submit your new patient intake form here, online. Web new patient intake form. Web fill out our new patient form to expedite the process and get your prescriptions faster from any of our new york city locations. Web online intake forms and practice management software from electronic forms and appointment scheduling to insurance billing and secure patient portals, everything you. All of our pharmacy locations accept electronic prescriptions. Web please consider sending your prescription electronically. Web new patient intake form how would you like us to contact you when your prescription is ready? Web credit card authorization form please print and complete all the information below. Web please consider sending your prescription electronically.
Speak with your personal physician about your. Web new patient intake form. Try the leading practice management solution for solo and group private practitioners. We want to help you get the best. Web please consider sending your prescription electronically. Web once we get this form, we will contact you and work with your pharmacy to transfer your medications, coordinate refills, and answer questions. All of our pharmacy locations accept electronic prescriptions. The form will need information such as patient information and. Ad register and subscribe now to work on your wellness pharmacy patient intake form. Ad digitize any existing form or easily create new forms to optimize patient experience.
Pharmacy Marketing Ideas Intake Forms
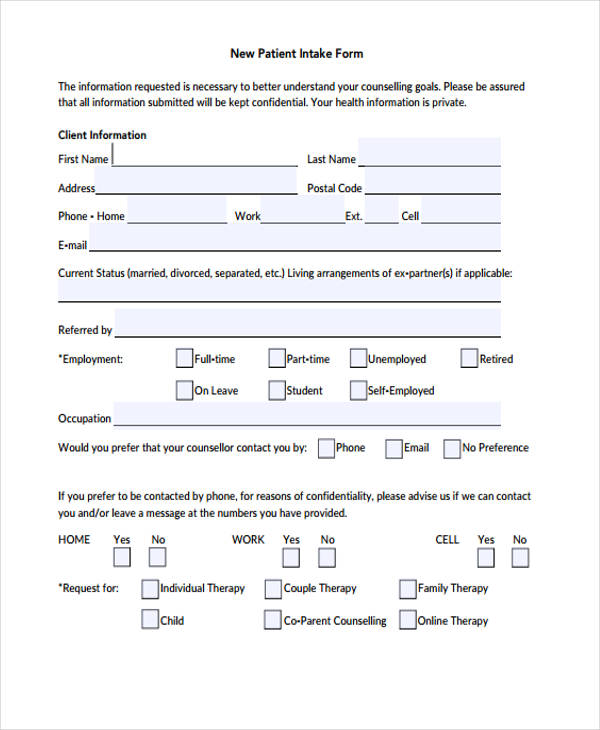
Web the objective of this form is to assist and help medical staff for keeping the records of used supplies by patients. We want to help you get the best. Web credit card authorization form please print and complete all the information below. Web every person's condition is unique and each patient requires a professional assessment before medical guidance can.

Addictionary
Simply select get started, fill out the form and submit. Web online intake forms and practice management software from electronic forms and appointment scheduling to insurance billing and secure patient portals, everything you. Web credit card authorization form please print and complete all the information below. Web that's why we offer a quick, simple way to submit your new patient.
FREE 9+ Medicine Patient Intake Forms in PDF MS Word
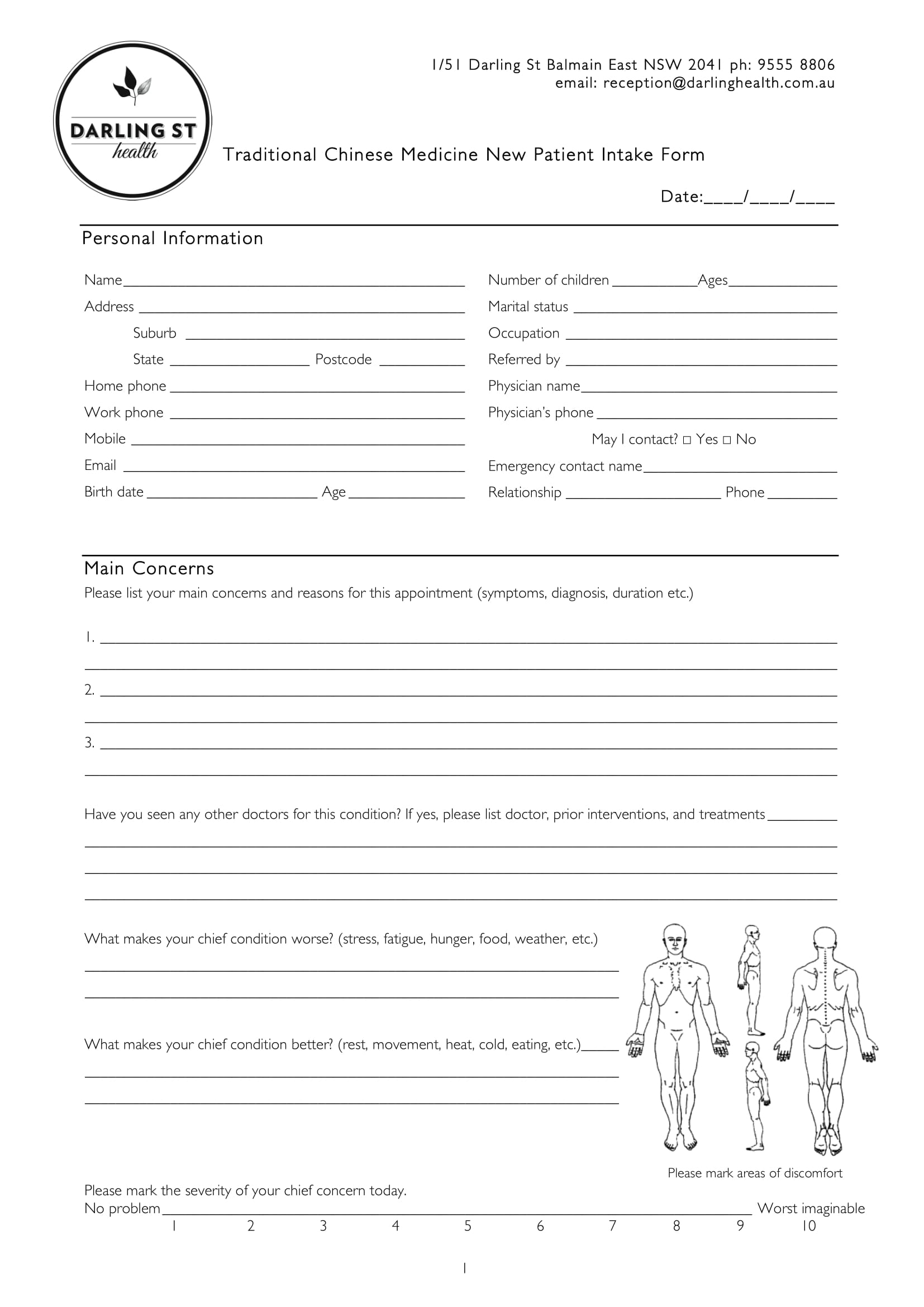
Web the objective of this form is to assist and help medical staff for keeping the records of used supplies by patients. Web 1964 new patient intake form name:____date of birth: The form will need information such as patient information and. Web every person's condition is unique and each patient requires a professional assessment before medical guidance can be given..
Patient Intake Form printable pdf download
Web online intake forms and practice management software from electronic forms and appointment scheduling to insurance billing and secure patient portals, everything you. At cvs specialty®, our goal is to help streamline the onboarding process to get. Web please consider sending your prescription electronically. Web send your specialty rx and enrollment form to us electronically, or by phone or fax..

New Patient Intake Form (Editable).pdf DocDroid
Ad register and subscribe now to work on your wellness pharmacy patient intake form. Web credit card authorization form please print and complete all the information below. Just complete this form, attach the original prescription(s), and mail it to us at the address shown below. Web every person's condition is unique and each patient requires a professional assessment before medical.
New Patient Intake Form printable pdf download
Web new patient intake form how would you like us to contact you when your prescription is ready? Simply select get started, fill out the form and submit. Web send your specialty rx and enrollment form to us electronically, or by phone or fax. Web the objective of this form is to assist and help medical staff for keeping the.
FREE 9+ Medicine Patient Intake Forms in PDF MS Word
Web 1964 new patient intake form name:____date of birth: Web new patient intake form. Ad register and subscribe now to work on your wellness pharmacy patient intake form. Web please consider sending your prescription electronically. Web please enter your date of birth to continue (mm/dd/yyyy) submit

Crosswind Pharmacy New Patient Intake Form Fill and Sign Printable
Speak with your personal physician about your. Web please consider sending your prescription electronically. Web once we get this form, we will contact you and work with your pharmacy to transfer your medications, coordinate refills, and answer questions. The form will need information such as patient information and. Ad digitize any existing form or easily create new forms to optimize.
FREE 48+ Counseling Forms in PDF MS Word
Web launch provider learning hub now. Simply select get started, fill out the form and submit. Web fill out our new patient form to expedite the process and get your prescriptions faster from any of our new york city locations. Web new patient intake form. Just complete this form, attach the original prescription(s), and mail it to us at the.

Patient confidentiality business plan
All of our pharmacy locations accept electronic prescriptions. All of our pharmacy locations accept electronic prescriptions. Web fill out our new patient form to expedite the process and get your prescriptions faster from any of our new york city locations. Web 1964 new patient intake form name:____date of birth: Web send your specialty rx and enrollment form to us electronically,.
Web Please Enter Your Date Of Birth To Continue (Mm/Dd/Yyyy) Submit
Web new patient intake form. All of our pharmacy locations accept electronic prescriptions. Web fill out our new patient form to expedite the process and get your prescriptions faster from any of our new york city locations. Ad register and subscribe now to work on your wellness pharmacy patient intake form.
Web Launch Provider Learning Hub Now.
Web online intake forms and practice management software from electronic forms and appointment scheduling to insurance billing and secure patient portals, everything you. Web 1964 new patient intake form name:____date of birth: We want to help you get the best. Web credit card authorization form please print and complete all the information below.
At Cvs Specialty®, Our Goal Is To Help Streamline The Onboarding Process To Get.
The form will need information such as patient information and. Simply select get started, fill out the form and submit. Web the objective of this form is to assist and help medical staff for keeping the records of used supplies by patients. Web every person's condition is unique and each patient requires a professional assessment before medical guidance can be given.
All Of Our Pharmacy Locations Accept Electronic Prescriptions.
Just complete this form, attach the original prescription(s), and mail it to us at the address shown below. Web once we get this form, we will contact you and work with your pharmacy to transfer your medications, coordinate refills, and answer questions. Speak with your personal physician about your. Web please consider sending your prescription electronically.