Medical Verification Form
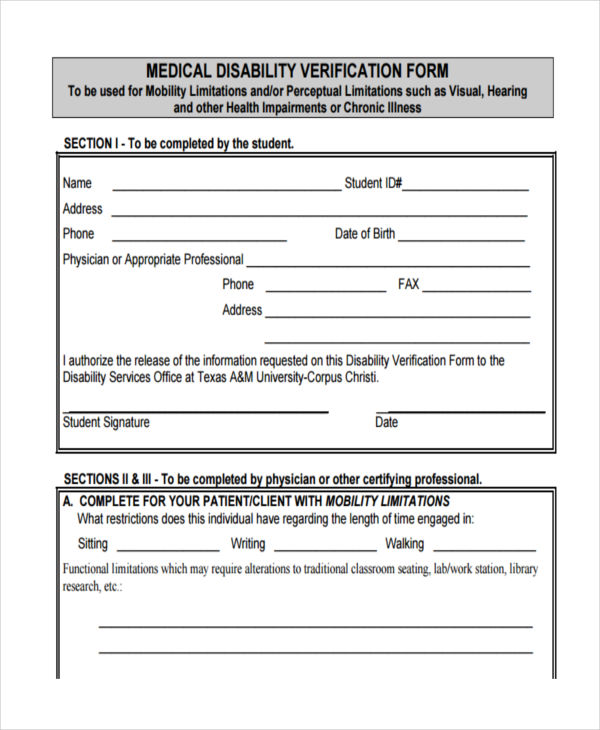
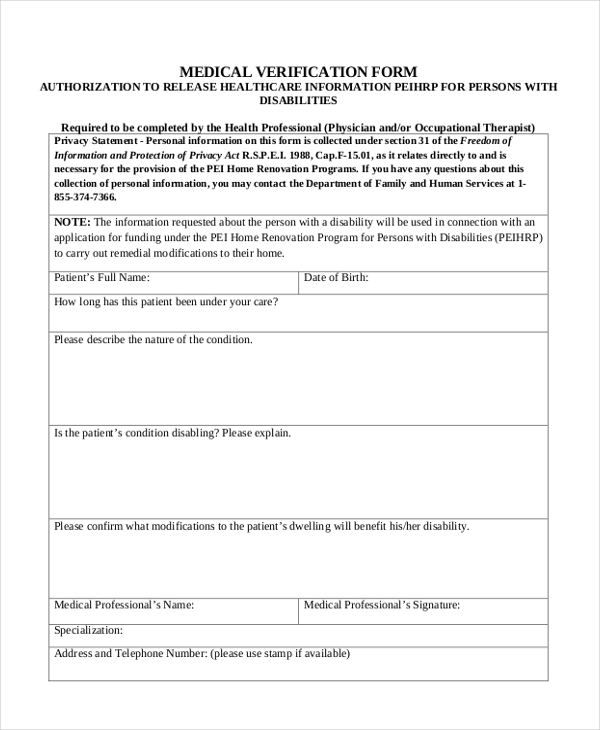
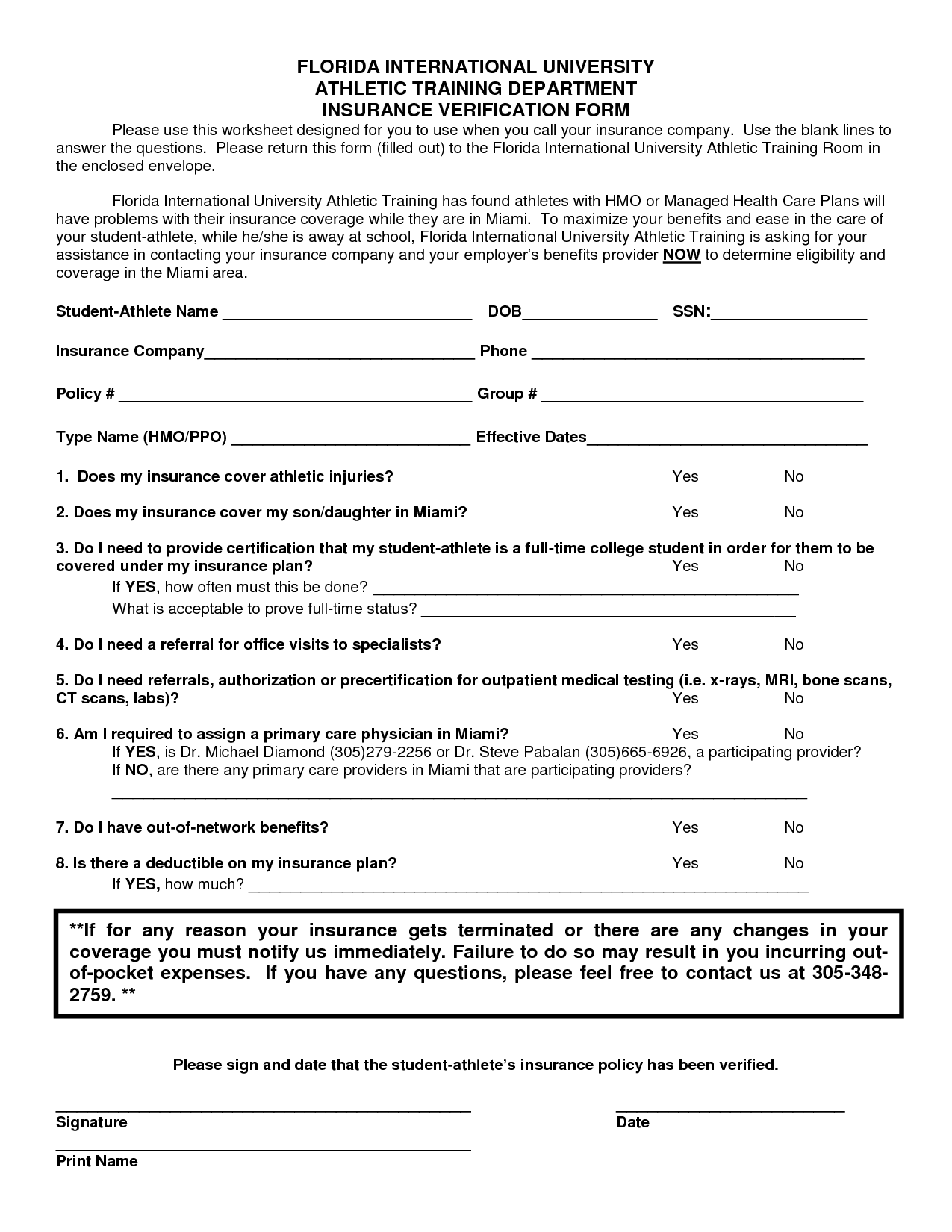
Medical Verification Form - Download and complete the verification of medical conditions form. Call or visit one of our release of information offices. Notice of denial of medical coverage/payment (integrated denial notice) Name of social worker/health care provider please. Health insurance premium payment program. Health insurance premium program (hipp) application. 1/1/21 v3) s21281 medical verification form page 3 of 7 a. Last 4 digits of social security number 3. A medical practitioner must complete this form. Web use this form to verify medical conditions affecting your capacity to work if you need an employment services assessment.
Health insurance premium payment program. Web use this form to verify medical conditions affecting your capacity to work if you need an employment services assessment. Download and complete the verification of medical conditions form. Web medical (health) insurance verification form. Web pass the national registry medical examiner certification test. A medical practitioner must complete this form. Patient information and medical release dcss 0020 (01/18/15) page 1 of 2 medical information verification report (physician's or psychologist's address, city state, zip code) (name of licensed physician or board certified psychologist) case. Notice of denial of medical coverage/payment (integrated denial notice) Once fmcsa has verified the medical examiner’s test score and validated his or her medical credential or license, the medical examiner is certified by fmcsa and listed on the national registry. Name of the household member for whom the accommodation is requested:
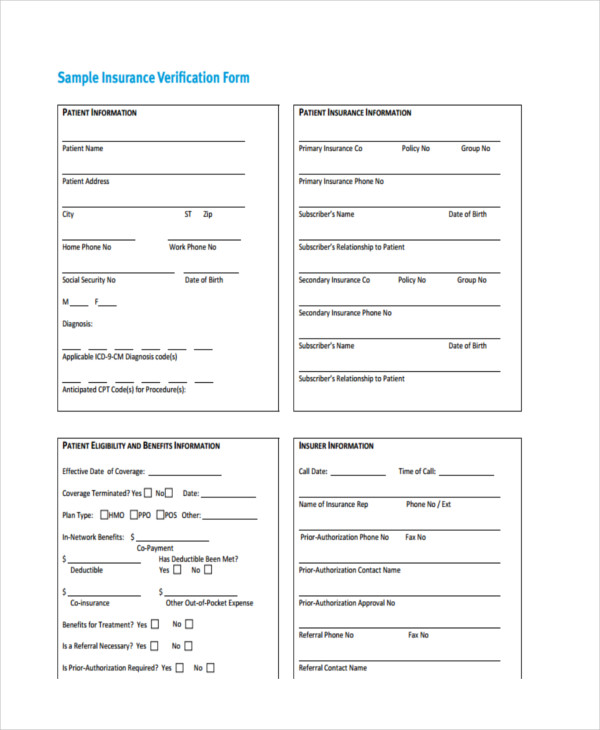
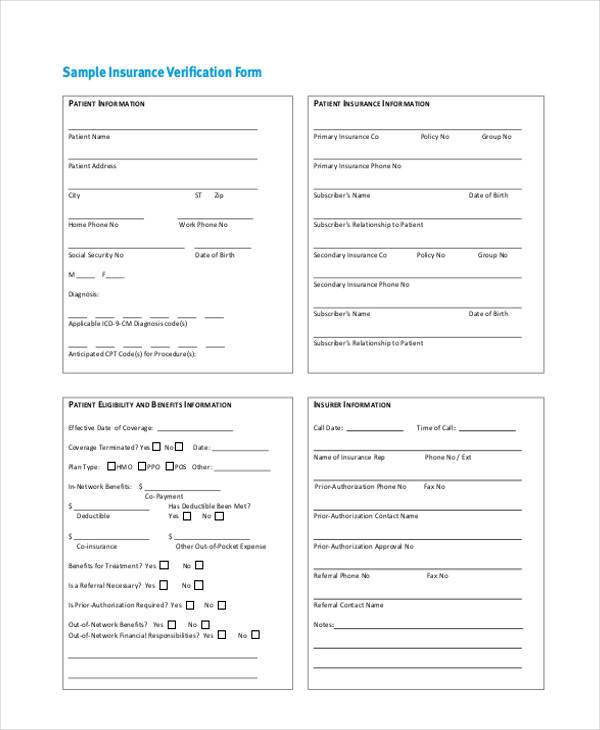
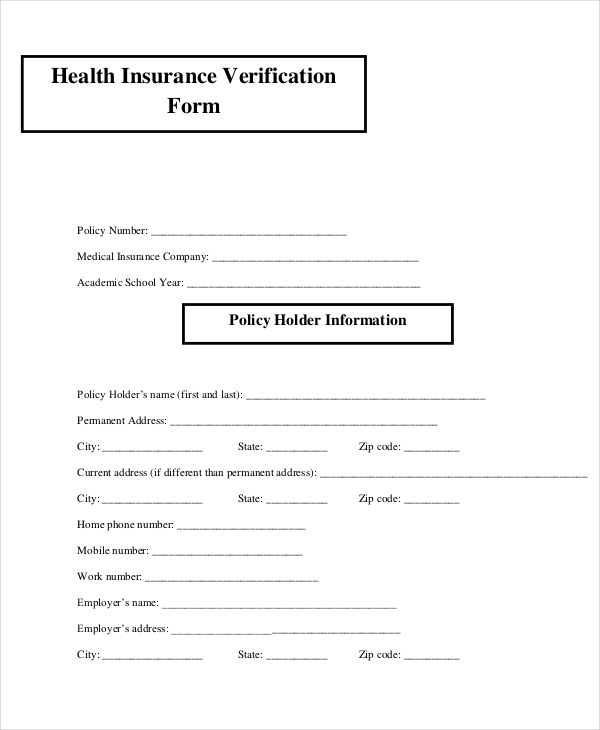
Form made fillable by eforms. An employee of the medical facility will be required to send the form to the patient’s insurance provider so that an agent may fill in the form. Web use this form to verify medical conditions affecting your capacity to work if you need an employment services assessment. Download and complete the verification of medical conditions form. Web estate recovery forms. The following provides access and/or information for many cms forms. Call or visit one of our release of information offices. Social worker/health care provider information 2. Patient information and medical release dcss 0020 (01/18/15) page 1 of 2 medical information verification report (physician's or psychologist's address, city state, zip code) (name of licensed physician or board certified psychologist) case. Web pass the national registry medical examiner certification test.
FREE 23+ Insurance Verification Forms in PDF
Dental, request for access to protected health information. Social worker/health care provider information 2. Once fmcsa has verified the medical examiner’s test score and validated his or her medical credential or license, the medical examiner is certified by fmcsa and listed on the national registry. Web cms forms list. A medical practitioner must complete this form.
FREE 8+ Medical Verification Forms in PDF
Dental, request for access to protected health information. Date of birth (mm/dd/yyyy) a translation of this document is available in your management office. Health care provider/social worker response 1. The following provides access and/or information for many cms forms. Last 4 digits of social security number 3.
FREE 44+ Medical Forms in PDF
Social worker/health care provider information 2. Dental, request for access to protected health information. A medical practitioner must complete this form. Date of birth (mm/dd/yyyy) a translation of this document is available in your management office. Web use this form to verify medical conditions affecting your capacity to work if you need an employment services assessment.
FREE 23+ Sample Verification Forms in PDF Word Excel
Download and complete the verification of medical conditions form. Once fmcsa has verified the medical examiner’s test score and validated his or her medical credential or license, the medical examiner is certified by fmcsa and listed on the national registry. Last 4 digits of social security number 3. Health care provider/social worker response 1. A medical insurance verification form is.
Medical Insurance Verification Form Template templates free printable
An employee of the medical facility will be required to send the form to the patient’s insurance provider so that an agent may fill in the form. Name of the household member for whom the accommodation is requested: Form made fillable by eforms. The following provides access and/or information for many cms forms. Health care provider/social worker response 1.
FREE 22+ Sample Medical Forms in PDF Excel Word
Health insurance premium payment program. An employee of the medical facility will be required to send the form to the patient’s insurance provider so that an agent may fill in the form. Web estate recovery forms. Web pass the national registry medical examiner certification test. The following provides access and/or information for many cms forms.
FREE 23+ Insurance Verification Forms in PDF MS Word
Call or visit one of our release of information offices. Web medical (health) insurance verification form. The following provides access and/or information for many cms forms. Patient information and medical release dcss 0020 (01/18/15) page 1 of 2 medical information verification report (physician's or psychologist's address, city state, zip code) (name of licensed physician or board certified psychologist) case. Name.
Free Medical (Health) Insurance Verification Form PDF eForms
Web medical (health) insurance verification form. Web we can also help you update your records. Health insurance premium program (hipp) application. A medical practitioner must complete this form. Social worker/health care provider information 2.
FREE 8+ Medical Verification Forms in PDF
Once fmcsa has verified the medical examiner’s test score and validated his or her medical credential or license, the medical examiner is certified by fmcsa and listed on the national registry. Download and complete the verification of medical conditions form. A medical insurance verification form is a document that a medical facility will use when verifying a patient’s medical coverage..
FREE 8+ Medical Verification Forms in PDF
Date of birth (mm/dd/yyyy) a translation of this document is available in your management office. Social worker/health care provider information 2. Web medical (health) insurance verification form. Download and complete the verification of medical conditions form. Notice of denial of medical coverage/payment (integrated denial notice)
The Following Provides Access And/Or Information For Many Cms Forms.
Call or visit one of our release of information offices. Name of social worker/health care provider please. Health care provider/social worker response 1. Web cms forms list.
Health Insurance Premium Program (Hipp) Application.
Last 4 digits of social security number 3. An employee of the medical facility will be required to send the form to the patient’s insurance provider so that an agent may fill in the form. Web use this form to verify medical conditions affecting your capacity to work if you need an employment services assessment. Social worker/health care provider information 2.
Patient Information And Medical Release Dcss 0020 (01/18/15) Page 1 Of 2 Medical Information Verification Report (Physician's Or Psychologist's Address, City State, Zip Code) (Name Of Licensed Physician Or Board Certified Psychologist) Case.
A medical practitioner must complete this form. Web estate recovery forms. Nformation patient name patient address city st zip home phone no work phone no social security no date of birth m f diagnosis: You may also use the search feature to more quickly locate information for a specific form number or form title.
Dental, Request For Access To Protected Health Information.
Date of birth (mm/dd/yyyy) a translation of this document is available in your management office. Once fmcsa has verified the medical examiner’s test score and validated his or her medical credential or license, the medical examiner is certified by fmcsa and listed on the national registry. Download and complete the verification of medical conditions form. Health insurance premium payment program.