Medical Information Request Form
Medical Information Request Form - To be completed by employee employer name: Web medical information request form purpose this form requests medical information for health conditions to determine reasonable accommodations. Web you may contact your current health care provider to have medical records sent to mayo clinic. Any information about prior treatment with a. Ad digitize any existing form or easily create new forms to optimize your patient experience. • the release of a minor child's medical records. Web mail or fax completed form to: Box 4087 austin, tx 78773 fax: Web to request release of medical information please complete and sign this form i, ____________________________________hereby voluntarily authorize. Like release of information forms, we do also produce medical.
Contact your mayo clinic care team to identify what types of records are needed,. Ad digitize any existing form or easily create new forms to optimize your patient experience. Medinfo@omeros.com if you are a us healthcare professional, you can submit your request by completing the form below. Web you may contact your current health care provider to have medical records sent to mayo clinic. Web medical information request form (mirf) 841 woburn street, wilmington, ma 01887, usa t. Web standard medical information release form. Web medical information request form please submit this form along with a hipaa release form section 1: Web medical information request form purpose this form requests medical information for health conditions to determine reasonable accommodations. Web to request release of medical information please complete and sign this form i, ____________________________________hereby voluntarily authorize. Web mail or fax completed form to:
Web mail or fax completed form to: Web do not use this form to request: Medinfo@omeros.com if you are a us healthcare professional, you can submit your request by completing the form below. Web submit a medical inquiry. _______________________ you must attach proof of your authority to act on. If you are a patient or caregiver and would like to. Ad digitize any existing form or easily create new forms to optimize your patient experience. Employees are to complete section i below, provide a copy of their job. Patients have the right to request a. Paratek is committed to providing timely and accurate information in response to unsolicited requests for scientific information regarding or.
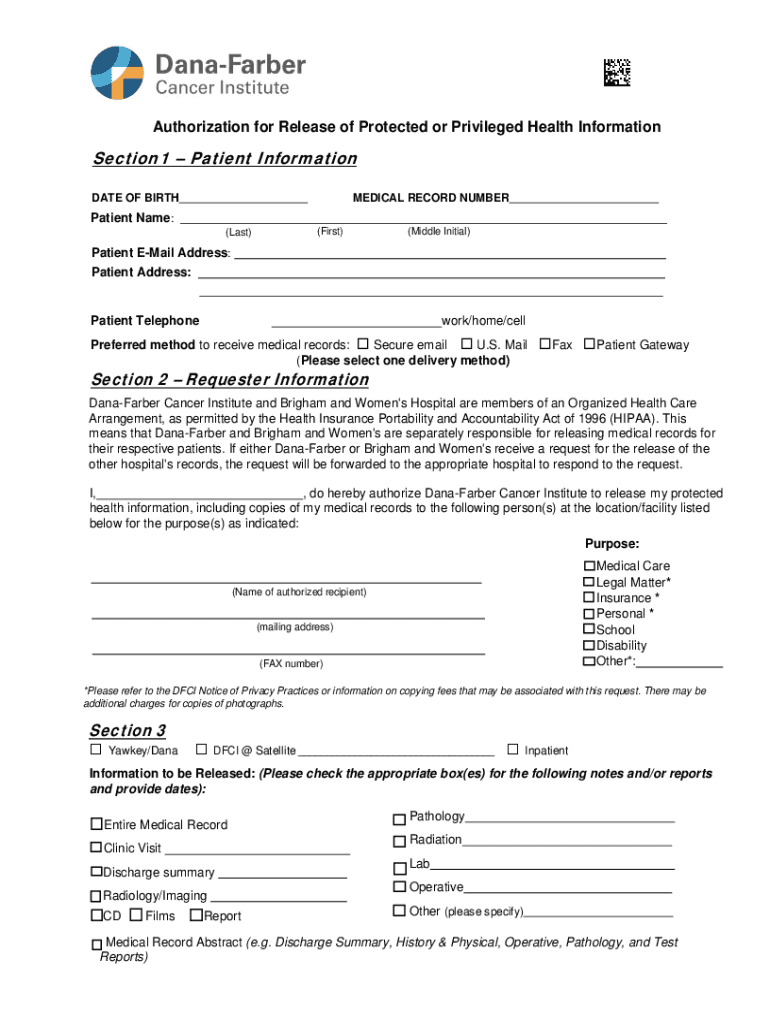
MA Dana Farber Cancer Institute Medical Information Request Form Fill
Web • the medical information request form is to be completed by the employee's physician or care provider. Web submit a medical inquiry. Texas department of public safety attn: Web to request release of medical information please complete and sign this form i, ____________________________________hereby voluntarily authorize. Web medical information request form purpose this form requests medical information for health conditions.
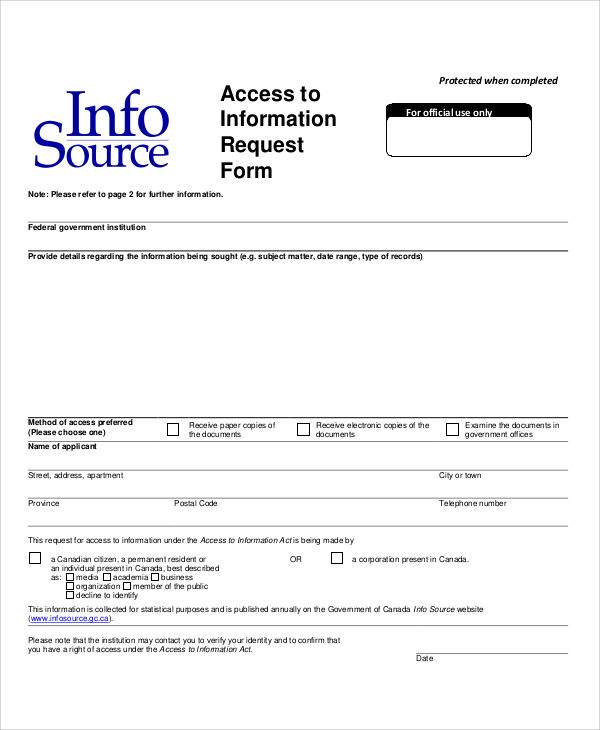
FREE 10+ Sample Information Request Forms in MS Word PDF
Web standard medical information release form. This form explains why the drug is needed so the insurance can approve its administration and use. Web health information request form please complete and return this form to your healthcare provider who will return this form to health current. Medinfo@omeros.com if you are a us healthcare professional, you can submit your request by.
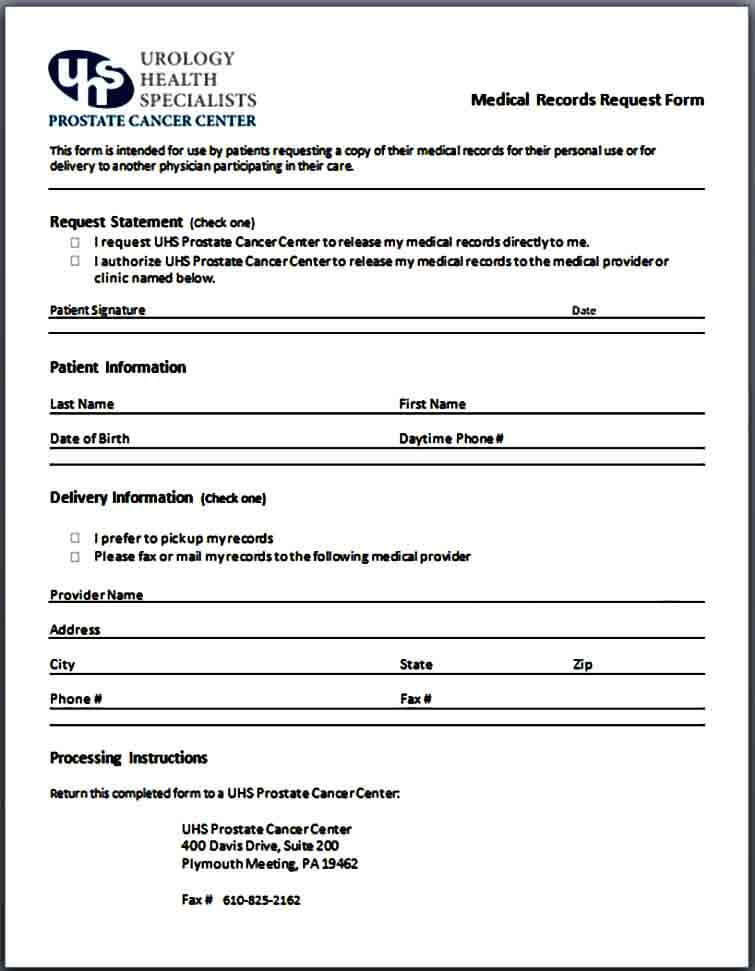
Sample Medical Records Request Form Mous Syusa
Web • the medical information request form is to be completed by the employee's physician or care provider. Web what’s it for? Employees are to complete section i below, provide a copy of their job. Web the application form, which will be available on the official etias website as well as a mobile application, has a fee of 7 euros.
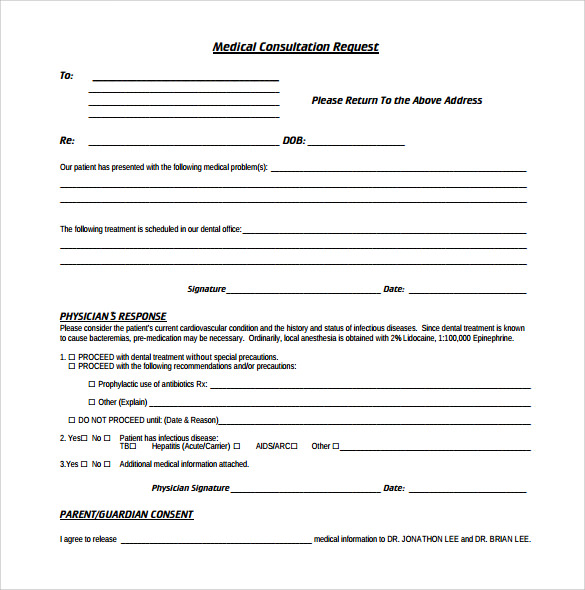
12 Medical Consultation Form Templates to Download Sample Templates
To submit your request, it is required that you select your country from the list below, then the form shall be displayed for you to complete. Web medical information request form (mirf) 841 woburn street, wilmington, ma 01887, usa t. Patients have the right to request a. Any information about prior treatment with a. Web health information request form please.

Health Records Application Letter Medical Records Request form
Answer simple questions to make a medical records request on any device in minutes. Web medical information (med info) request form home medinfo medinfo form medical information (med info) request form please complete the form below country. Web to request release of medical information please complete and sign this form i, ____________________________________hereby voluntarily authorize. Web you may contact your current.
FREE 10+ Sample Information Request Forms in MS Word PDF
Web mail or fax completed form to: Web you may contact your current health care provider to have medical records sent to mayo clinic. Web to request release of medical information please complete and sign this form i, ____________________________________hereby voluntarily authorize. Web health information request form please complete and return this form to your healthcare provider who will return this.

Medical Records Request Form download free documents for PDF, Word
Web medical information request form (mirf) 841 woburn street, wilmington, ma 01887, usa t. If you are a patient or caregiver and would like to. Web standard medical information release form. Ad digitize any existing form or easily create new forms to optimize your patient experience. Web medical information request form purpose this form requests medical information for health conditions.
Personal Information Medical Term
Box 4087 austin, tx 78773 fax: Web mail or fax completed form to: Web medical information request form purpose this form requests medical information for health conditions to determine reasonable accommodations. • the release of a minor child's medical records. Like release of information forms, we do also produce medical.

Sample Medical Records Request Form Medical records, Medical, Medical
Web medical information request form please submit this form along with a hipaa release form section 1: Texas department of public safety attn: Paratek is committed to providing timely and accurate information in response to unsolicited requests for scientific information regarding or. _______________________ you must attach proof of your authority to act on. If you are a patient or caregiver.
Medical Records Request Form in Word and Pdf formats
Use this va form to authorize va to share your health information with a. Ad digitize any existing form or easily create new forms to optimize your patient experience. Medinfo@omeros.com if you are a us healthcare professional, you can submit your request by completing the form below. To be completed by employee employer name: If you are a patient or.
• The Release Of A Minor Child's Medical Records.
Web by checking this box and typing my name, i hereby confirm that the medical information and/or inquiry requested was at my initiation and was not solicited in any manner by a. Texas department of public safety attn: Box 4087 austin, tx 78773 fax: Any information about prior treatment with a.
Web Medical Information Request Form Purpose This Form Requests Medical Information For Health Conditions To Determine Reasonable Accommodations.
Web medical information request form (mirf) 841 woburn street, wilmington, ma 01887, usa t. Answer simple questions to make a medical records request on any device in minutes. Web to request release of medical information please complete and sign this form i, ____________________________________hereby voluntarily authorize. Web standard medical information release form.
Web Submit A Medical Inquiry.
Like release of information forms, we do also produce medical. Web medical information (med info) request form home medinfo medinfo form medical information (med info) request form please complete the form below country. If you're a mayo clinic health system patient or have been one in the past, you can use these forms to grant permission for others to access your protected. If you are a patient or caregiver and would like to.
To Be Completed By Employee Employer Name:
Web mail or fax completed form to: Patients have the right to request a. Web • the medical information request form is to be completed by the employee's physician or care provider. To submit your request, it is required that you select your country from the list below, then the form shall be displayed for you to complete.