Medicaid Tubal Consent Form
Medicaid Tubal Consent Form - Resident name* date of birth medicaid number*. Develop a standardized, validated decision support tool. The first section of the form requires you to provide your name,. The beneficiary must be 21. Web form 392 : Name of the sterilization procedure to be performed (e.g., tubal ligation or vasectomy). Web this form allows an individual to provide consent for sterilization. Web sterilization consent form hospital/clinic notice: Web up to $40 cash back here are the steps to fill out the ohio medicaid sterilization consent form: Your decision at any time to be sterilized will not result in the.
Your decision at any time to be sterilized will not result in the. Develop a standardized, validated decision support tool. The beneficiary must be 21. Web form 392 : Name of the sterilization procedure to be performed (e.g., tubal ligation or vasectomy). Statements are also included for an interpreter, a person obtaining consent, and a physician. Beneficiary’s complete birth date (month, day, and year). Resident name* date of birth medicaid number*. Web this bulletin replaces updated sterilization consent form published on feb. Web alabama medicaid agency sterilization consent form notice:
Statements are also included for an interpreter, a person obtaining consent, and a physician. The first section of the form requires you to provide your name,. Name of the sterilization procedure to be performed (e.g., tubal ligation or vasectomy). Web options to address medicaid consent policy. Web alabama medicaid agency sterilization consent form notice: Develop a standardized, validated decision support tool. Web the cost of a tubal ligation varies and depends on where you get it, what kind you get, and whether or not you have health insurance that will cover some or all of the cost. Web sterilization consent form hospital/clinic notice: 14, 2023, to update dates providers should be using each consent form. Resident name* date of birth medicaid number*.

2010 Form HHS687 Fill Online, Printable, Fillable, Blank pdfFiller
Complete and distribute copies to: Web this bulletin replaces updated sterilization consent form published on feb. Web nc medicaid recommends providers with beneficiaries who have signed consents close to 150 days post signature, with potential for surgery delay, have those. Web providers can access the sterilization consent form by clicking on the words “sterilization consent form.”. Web alabama medicaid agency.
Tubal Ligation Consent Form Printable Consent Form
Web the cost of a tubal ligation varies and depends on where you get it, what kind you get, and whether or not you have health insurance that will cover some or all of the cost. Web this bulletin replaces updated sterilization consent form published on feb. Beneficiary’s complete birth date (month, day, and year). Web nc medicaid recommends providers.

Medicaid Tubal Ligation Consent Form 2022 Printable Consent Form 2022
Web the cost of a tubal ligation varies and depends on where you get it, what kind you get, and whether or not you have health insurance that will cover some or all of the cost. Providers may choose to complete the form for. Web providers can access the sterilization consent form by clicking on the words “sterilization consent form.”..

Pm 284 Form Fill Online, Printable, Fillable, Blank pdfFiller
See if you're eligible for freedomcare® program. Web nc medicaid recommends providers with beneficiaries who have signed consent forms close to 150 days old have those beneficiaries resign tubal sterilization. Web because these policies have not changed since 1978, women requesting publicly funded sterilization must complete the “consent to sterilization” section of the. Web voluntary tubal ligation is legal in.
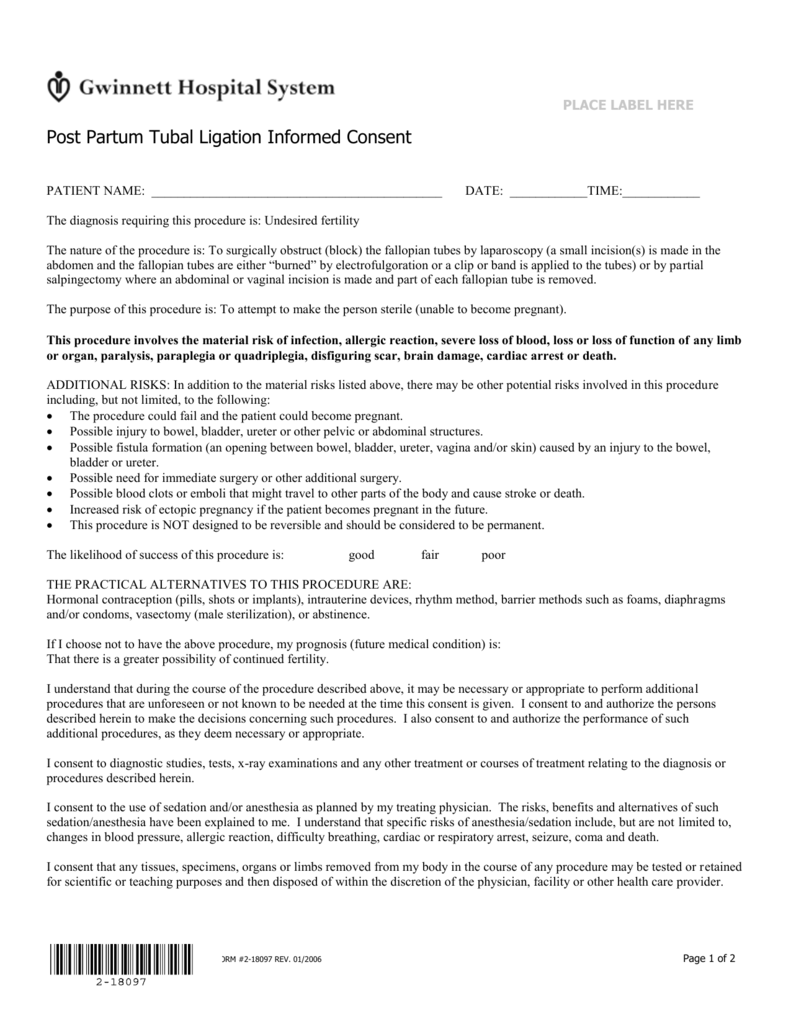
Post Partum Tubal Ligation Informed Consent English
Providers may choose to complete the form for. The beneficiary must be 21. Web alabama medicaid agency sterilization consent form notice: See if you're eligible for freedomcare® program. 14, 2023, to update dates providers should be using each consent form.

Medicaid needs to change its rules for women seeking tubal ligation STAT
Complete and distribute copies to: Web nc medicaid recommends providers with beneficiaries who have signed consent forms close to 150 days old have those beneficiaries resign tubal sterilization. The beneficiary must be 21. Providers may choose to complete the form for. Web transition to community referral form asterisk (*) denotes required fields date of admission* referral date*.

Will Medicaid Pay For Tubal Reversal?
The first section of the form requires you to provide your name,. Web nc medicaid recommends providers with beneficiaries who have signed consents close to 150 days post signature, with potential for surgery delay, have those. Resident name* date of birth medicaid number*. The #1 home care program in missouri. Name of the sterilization procedure to be performed (e.g., tubal.
Medicaid Consent Form Suwannee County Schools Printable Free Nude
Web this bulletin replaces updated sterilization consent form published on feb. Web nc medicaid recommends providers with beneficiaries who have signed consents close to 150 days post signature, with potential for surgery delay, have those. 14, 2023, to update dates providers should be using each consent form. The #1 home care program in missouri. Web form 392 :

Tubal Ligation Consent Form Printable Consent Form
Web this form allows an individual to provide consent for sterilization. Web because these policies have not changed since 1978, women requesting publicly funded sterilization must complete the “consent to sterilization” section of the. Redefine the validity time frame to a minimum of 24 hours extending up to 1. Your decision at any time not to be sterilized will not.

Will Medicaid Pay For Tubal Reversal?
Complete and distribute copies to: Web alabama medicaid agency sterilization consent form notice: Web the cost of a tubal ligation varies and depends on where you get it, what kind you get, and whether or not you have health insurance that will cover some or all of the cost. Beneficiary’s complete birth date (month, day, and year). Providers may choose.
Web This Bulletin Replaces Updated Sterilization Consent Form Published On Feb.
Web nc medicaid recommends providers with beneficiaries who have signed consent forms close to 150 days old have those beneficiaries resign tubal sterilization. Redefine the validity time frame to a minimum of 24 hours extending up to 1. Web form 392 : Web nc medicaid recommends providers with beneficiaries who have signed consents close to 150 days post signature, with potential for surgery delay, have those.
Statements Are Also Included For An Interpreter, A Person Obtaining Consent, And A Physician.
Web alabama medicaid agency sterilization consent form notice: See if you're eligible for freedomcare® program. Web sterilization consent form instructions: Web transition to community referral form asterisk (*) denotes required fields date of admission* referral date*.
Web Up To $40 Cash Back Here Are The Steps To Fill Out The Ohio Medicaid Sterilization Consent Form:
Providers may choose to complete the form for. The beneficiary must be 21. Web sterilization consent form hospital/clinic notice: Your decision at any time to be sterilized will not result in the.
Web The Cost Of A Tubal Ligation Varies And Depends On Where You Get It, What Kind You Get, And Whether Or Not You Have Health Insurance That Will Cover Some Or All Of The Cost.
Name of the sterilization procedure to be performed (e.g., tubal ligation or vasectomy). Ad pay trusted family/friends to care for you, get started with freedomcare® today. Beneficiary’s complete birth date (month, day, and year). Complete and distribute copies to: