Ilumya Enrollment Form Pdf
Ilumya Enrollment Form Pdf - 2.2 tuberculosis assessment prior to initiation of ilumya Save or instantly send your ready documents. Contact your field reimbursement manager with any questions about prescribing ilumya™. Check out how easy it is to complete and esign documents online using fillable templates and a powerful editor. Patient financial information (only complete this section if requesting the patient assistance program) us resident? £ yes £ no disabled (longer than 2 years)? Confirm we will confirm if your prescription is covered by your insurance provider and if you are qualified for ilumya ® financial support programs. Web complete ilumya enrollment form online with us legal forms. Easily fill out pdf blank, edit, and sign them. The recommended dose is 100 mg at weeks 0, 4, and every twelve weeks thereafter.
The recommended dose is 100 mg at weeks 0, 4, and every twelve weeks thereafter. Web if you are not the patient or the prescriber, you will need to submit a phi disclosure authorization form with this request which can be found at the following link: Easily fill out pdf blank, edit, and sign them. Web start enrollment through the ilumya ® provider portal or by completing an ilumya support ® patient services enrollment form. 2.2 tuberculosis assessment prior to initiation of ilumya £ yes £ no disabled (longer than 2 years)? Use this guide to ensure your form is fully and accurately completed. Web ilumya support enrollment form. Prescriber information patient first name patient last name first name last name date of birth (dd/mm/yyyy) Get everything done in minutes.
Please complete this form in its entirety by providing the following information: Web the ilumya support™ enrollment form is the first step to getting your patients started with our comprehensive patient services. Save or instantly send your ready documents. The recommended dose is 100 mg at weeks 0, 4, and every twelve weeks thereafter. £ yes £ no disabled (longer than 2 years)? Use this guide to ensure your form is fully and accurately completed. Prescriber information patient first name patient last name first name last name date of birth (dd/mm/yyyy) 2.2 tuberculosis assessment prior to initiation of ilumya Please complete all fields to minimize delays. Web start enrollment through the ilumya ® provider portal or by completing an ilumya support ® patient services enrollment form.
Generic Ach Enrollment Form Form Resume Examples mL52p6KkXo
Patient financial information (only complete this section if requesting the patient assistance program) us resident? Web complete ilumya enrollment form online with us legal forms. Confirm we will confirm if your prescription is covered by your insurance provider and if you are qualified for ilumya ® financial support programs. Save or instantly send your ready documents. Contact your field reimbursement.

Ilumya (tildrakizumab) BC SUN PSP Form 092022 Juno EMR Support Portal
£ yes £ no disabled (longer than 2 years)? Check out how easy it is to complete and esign documents online using fillable templates and a powerful editor. Web the ilumya support™ enrollment form is the first step to getting your patients started with our comprehensive patient services. Patient financial information (only complete this section if requesting the patient assistance.
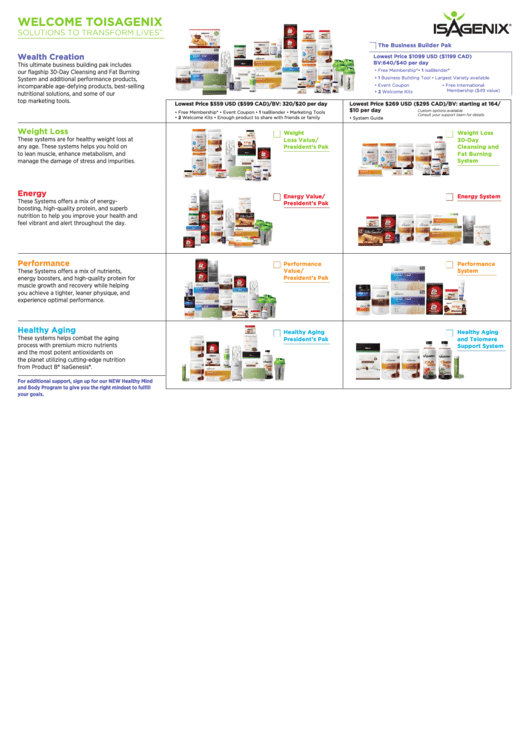
Fillable Isagenix Enrollment Form printable pdf download
Patient financial information (only complete this section if requesting the patient assistance program) us resident? Prescriber information patient first name patient last name first name last name date of birth (dd/mm/yyyy) Contact your field reimbursement manager with any questions about prescribing ilumya™. Get everything done in minutes. Web start enrollment through the ilumya ® provider portal or by completing an.

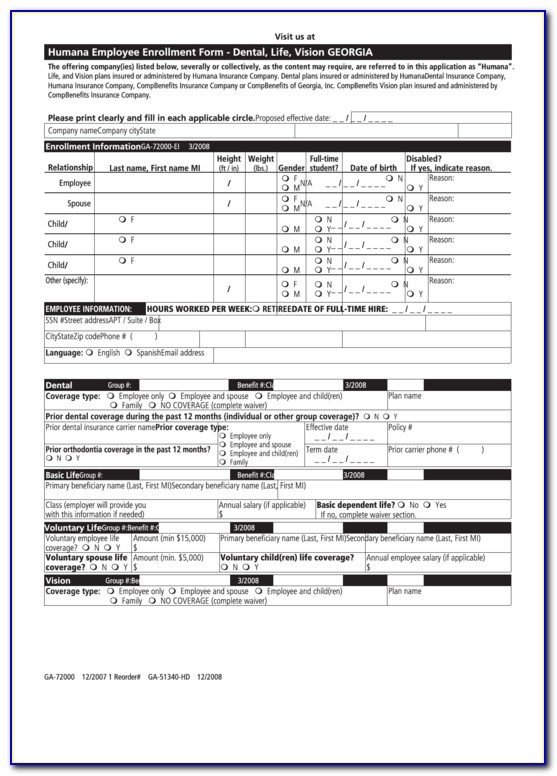
Humana Enrollment Form Pdf Fill Online, Printable, Fillable, Blank
The recommended dose is 100 mg at weeks 0, 4, and every twelve weeks thereafter. Confirm we will confirm if your prescription is covered by your insurance provider and if you are qualified for ilumya ® financial support programs. Please complete all fields to minimize delays. Web ilumya support enrollment form. Send this completed form to sun pharma by one.
![[Printable] Basic Education Enrollment Form of DepEd](http://governmentph.com/wp-content/uploads/2020/01/DepEd-Basic-Education-Enrollment-Form.jpg)
[Printable] Basic Education Enrollment Form of DepEd
Please complete all fields to minimize delays. Web ilumya is administered by subcutaneous injection. Check out how easy it is to complete and esign documents online using fillable templates and a powerful editor. Contact your field reimbursement manager with any questions about prescribing ilumya™. Send this completed form to sun pharma by one of the following ways:.

Ilumya Enrollment Form Fill and Sign Printable Template Online US
Web ilumya support enrollment form. Web ilumya is administered by subcutaneous injection. Contact your field reimbursement manager with any questions about prescribing ilumya™. Web if you are not the patient or the prescriber, you will need to submit a phi disclosure authorization form with this request which can be found at the following link: Prescriber information patient first name patient.

Sample Ach Enrollment Form Form Resume Examples goVLPd3Vva
Use this guide to ensure your form is fully and accurately completed. Please complete all fields to minimize delays. Confirm we will confirm if your prescription is covered by your insurance provider and if you are qualified for ilumya ® financial support programs. £ yes £ no disabled (longer than 2 years)? Web complete ilumya enrollment form online with us.

VIP Enrollment Form.pdf DocDroid
Web this enrollment form to purchase ilumya™ through our buy and bill program. The recommended dose is 100 mg at weeks 0, 4, and every twelve weeks thereafter. Easily fill out pdf blank, edit, and sign them. Use this guide to ensure your form is fully and accurately completed. Save or instantly send your ready documents.
Wellcare Value Script Enrollment Form Form Resume Examples EZVgRlkYJk
Web the ilumya support™ enrollment form is the first step to getting your patients started with our comprehensive patient services. Easily fill out pdf blank, edit, and sign them. Get everything done in minutes. Please complete this form in its entirety by providing the following information: Confirm we will confirm if your prescription is covered by your insurance provider and.

23+ Free Appeal Letter Template Format, Sample & Example Best
Patient financial information (only complete this section if requesting the patient assistance program) us resident? Please complete this form in its entirety by providing the following information: Get everything done in minutes. 2.2 tuberculosis assessment prior to initiation of ilumya Web start enrollment through the ilumya ® provider portal or by completing an ilumya support ® patient services enrollment form.
Save Or Instantly Send Your Ready Documents.
Web start enrollment through the ilumya ® provider portal or by completing an ilumya support ® patient services enrollment form. Confirm we will confirm if your prescription is covered by your insurance provider and if you are qualified for ilumya ® financial support programs. Send this completed form to sun pharma by one of the following ways:. Web the ilumya support™ enrollment form is the first step to getting your patients started with our comprehensive patient services.
Web Ilumya Is Administered By Subcutaneous Injection.
Web complete ilumya enrollment form online with us legal forms. Check out how easy it is to complete and esign documents online using fillable templates and a powerful editor. Get everything done in minutes. Please complete this form in its entirety by providing the following information:
Web If You Are Not The Patient Or The Prescriber, You Will Need To Submit A Phi Disclosure Authorization Form With This Request Which Can Be Found At The Following Link:
Web ilumya support enrollment form. Web ask your dermatologist to submit your ilumya support lighting the way ® enrollment form so that you can receive all the benefits available to you. Please complete all fields to minimize delays. £ yes £ no disabled (longer than 2 years)?
2.2 Tuberculosis Assessment Prior To Initiation Of Ilumya
Patient financial information (only complete this section if requesting the patient assistance program) us resident? Use this guide to ensure your form is fully and accurately completed. Easily fill out pdf blank, edit, and sign them. Prescriber information patient first name patient last name first name last name date of birth (dd/mm/yyyy)