Eyemed Out Of Network Form
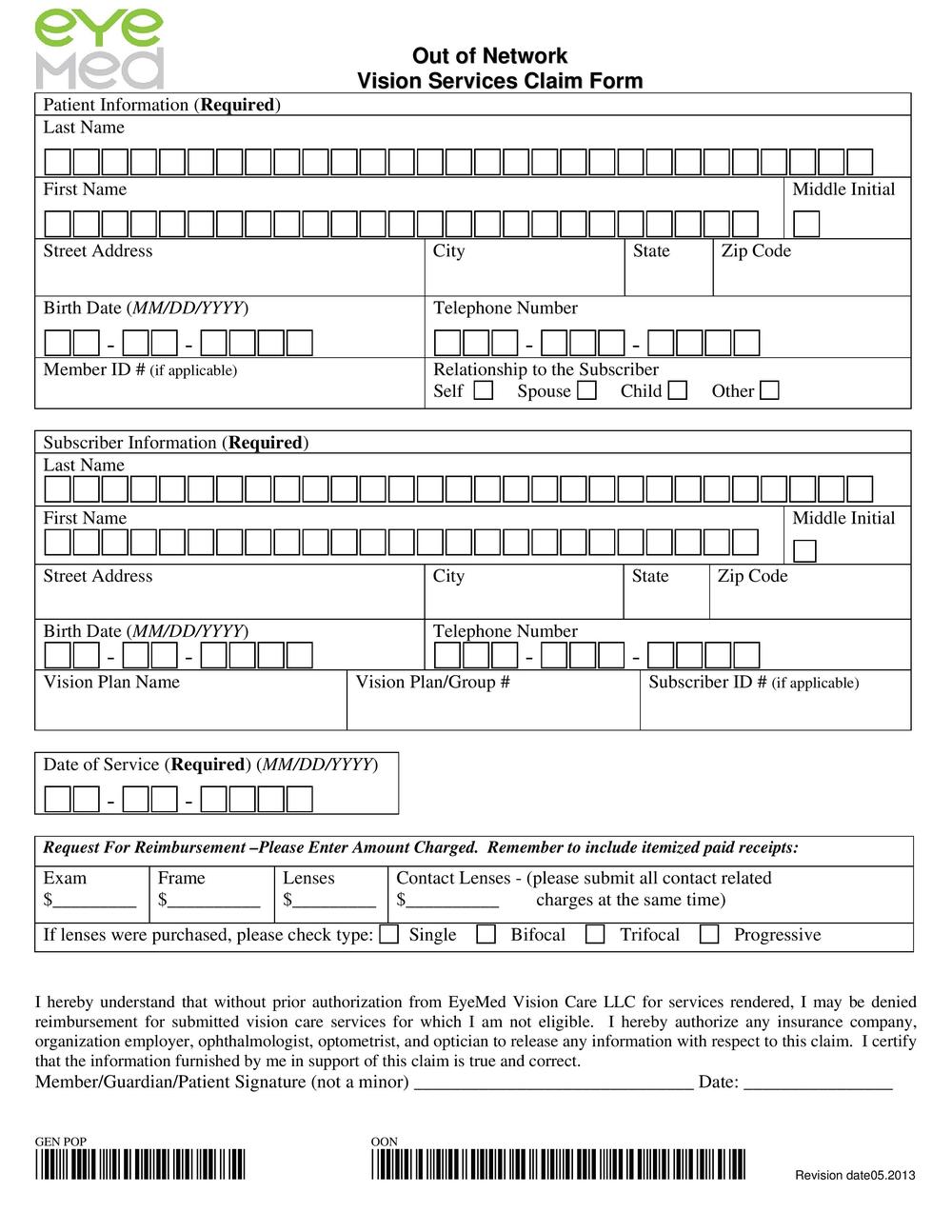
Eyemed Out Of Network Form - Claim form, vision, vision certificate. Patient and subscriber information last name first name date of birth street address city state zip code 2. You can now submit your form online or by mail: Go green and get paid faster. Web eyemed out of network claim form. Eyemed will reimburse you for authorized services according to your plan design. Please complete all sections of this form to ensure proper benefit allocation. Please complete and send this form to eyemed within the period of time specified by your plan. Any missing or incomplete information may result in delay of payment or the form being returned. One of the following exceptions must apply, based on your home or work address:
You can now submit your form online or by mail: Based from your home or office location, you were unable to: Patient and subscriber information last name first name date of birth street address city state zip code 2. One of the following exceptions must apply, based on your home or work address: Any missing or incomplete information may result in delay of payment or the form being returned. Please complete and send this form to eyemed within the period of time specified by your plan. Click below to complete an electronic claim form. Doctor or store information name street. You can now submit your form online or by mail: Click below to complete an electronic claim form.
Web eyemed out of network claim form. You can now submit your form online or by mail: You can now submit your form online or by mail: Go green and get paid faster. Based from your home or office location, you were unable to: Patient and subscriber information last name first name date of birth street address city state zip code 2. You can now submit your form online or by mail: Please complete and send this form to eyemed within the period of time specified by your plan. Go green and get paid faster. Any missing or incomplete information may result in delay of payment or the form being returned.

Eyemed Insurance Out Of Network Claim Form Creativmakeup Co
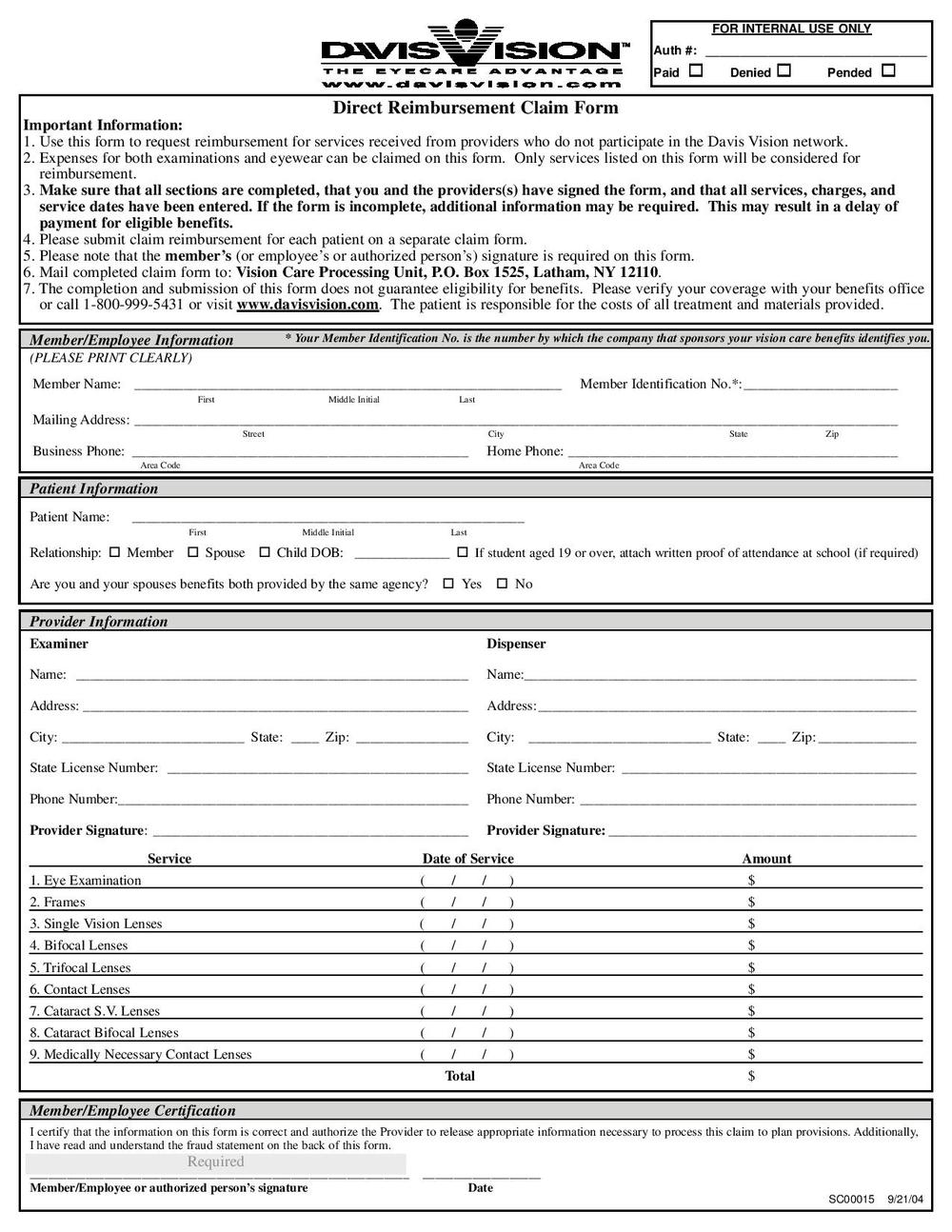
Based from your home or office location, you were unable to: You must submit a claim form to eyemed for reimbursement. Claim form, vision, vision certificate. Click below to complete an electronic claim form. Eyemed will reimburse you for authorized services according to your plan design.
Drs. Robert Stahl & Amy Calder, Optometrists Blog
Please complete and send this form to eyemed within the period of time specified by your plan. Click below to complete an electronic claim form. Online click below to complete an electronic claim form. Go green and get paid faster. Go green and get paid faster.
Drs. Robert Stahl & Amy Calder, Optometrists Blog
Doctor or store information name street. Any missing or incomplete information may result in delay of payment or the form being returned. Go green and get paid faster. Click below to complete an electronic claim form. Patient and subscriber information last name first name date of birth street address city state zip code 2.

EyeMed Insurance "Out of Network" claim form by Drs. Stahl & Calder Issuu
Doctor or store information name street. Click below to complete an electronic claim form. You must submit a claim form to eyemed for reimbursement. Go green and get paid faster. Claim form, vision, vision certificate.
Insurance Information Tuttle & Sawmill Eye Associates, Dublin OH
Please complete and send this form to eyemed within the period of time specified by your plan. You must submit a claim form to eyemed for reimbursement. Patient and subscriber information last name first name date of birth street address city state zip code 2. One of the following exceptions must apply, based on your home or work address: You.

Media Tweets by EyeMed Vision Care (EyeMedVision) Twitter
Eyemed will reimburse you for authorized services according to your plan design. Patient and subscriber information last name first name date of birth street address city state zip code 2. One of the following exceptions must apply, based on your home or work address: Doctor or store information name street. Please complete all sections of this form to ensure proper.

Eyemed enrollment form Fill out & sign online DocHub
You must submit a claim form to eyemed for reimbursement. Doctor or store information name street. Based from your home or office location, you were unable to: Click below to complete an electronic claim form. Online click below to complete an electronic claim form.
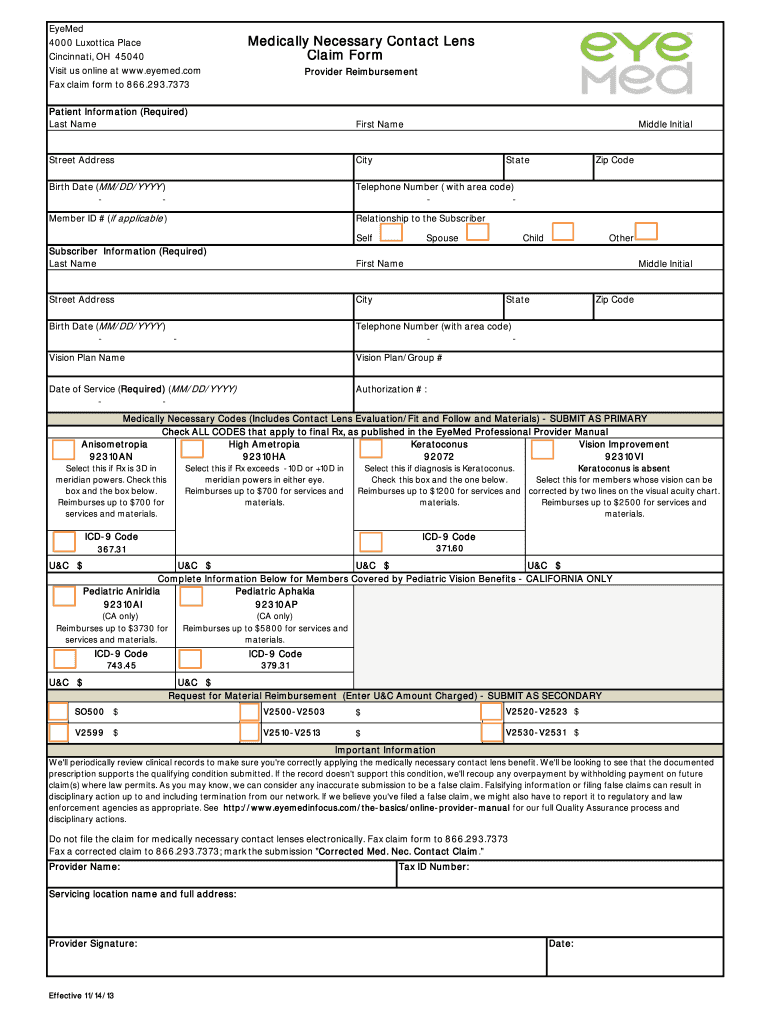
Eyemed Medically Necessary Contacts Fill Online, Printable, Fillable
Online click below to complete an electronic claim form. You can now submit your form online or by mail: Claim form, vision, vision certificate. Click below to complete an electronic claim form. Doctor or store information name street.

Out Of Network Vision Services Claim Form 2013 Printable Pdf Download
Doctor or store information name street. Any missing or incomplete information may result in delay of payment or the form being returned. Go green and get paid faster. Web eyemed out of network claim form. Online click below to complete an electronic claim form.
Eyemed Claim Form ≡ Fill Out Printable PDF Forms Online
Patient and subscriber information last name first name date of birth street address city state zip code 2. Go green and get paid faster. Doctor or store information name street. Please complete and send this form to eyemed within the period of time specified by your plan. You must submit a claim form to eyemed for reimbursement.
Based From Your Home Or Office Location, You Were Unable To:
Online click below to complete an electronic claim form. Click below to complete an electronic claim form. Claim form, vision, vision certificate. You can now submit your form online or by mail:
Eyemed Will Reimburse You For Authorized Services According To Your Plan Design.
Doctor or store information name street. Please complete and send this form to eyemed within the period of time specified by your plan. You can now submit your form online or by mail: Web eyemed out of network claim form.
Go Green And Get Paid Faster.
Patient and subscriber information last name first name date of birth street address city state zip code 2. Please complete all sections of this form to ensure proper benefit allocation. Any missing or incomplete information may result in delay of payment or the form being returned. Click below to complete an electronic claim form.
One Of The Following Exceptions Must Apply, Based On Your Home Or Work Address:
You can now submit your form online or by mail: Go green and get paid faster. You must submit a claim form to eyemed for reimbursement.