Emergency Medical Treatment Authorization Form
Emergency Medical Treatment Authorization Form - Edit & print for immediate use. Web emergency medical treatment authorization form this form grants temporary authority to a designated school official to provide and arrange for medical care for a minor who is a. Ill or involved in an. This form gran ts temporary au thority to largo l earning aca demy as designated to provide and a rrange for m edical. Get form templates for any purpose! Complete and use in under 10 minutes. Web emergency and medical treatment authorization authorization , has permission to take the following actions that i have checked yes. Web building inspection form (center in a residence) building inspection form (change of ownership/continued use) change of information form (coi) for cbc portal. Web in the event reasonable attempts to contact me have been unsuccessful, i hereby give my consent for: (name of child) for the period _____ to _____ to arrange for routine.
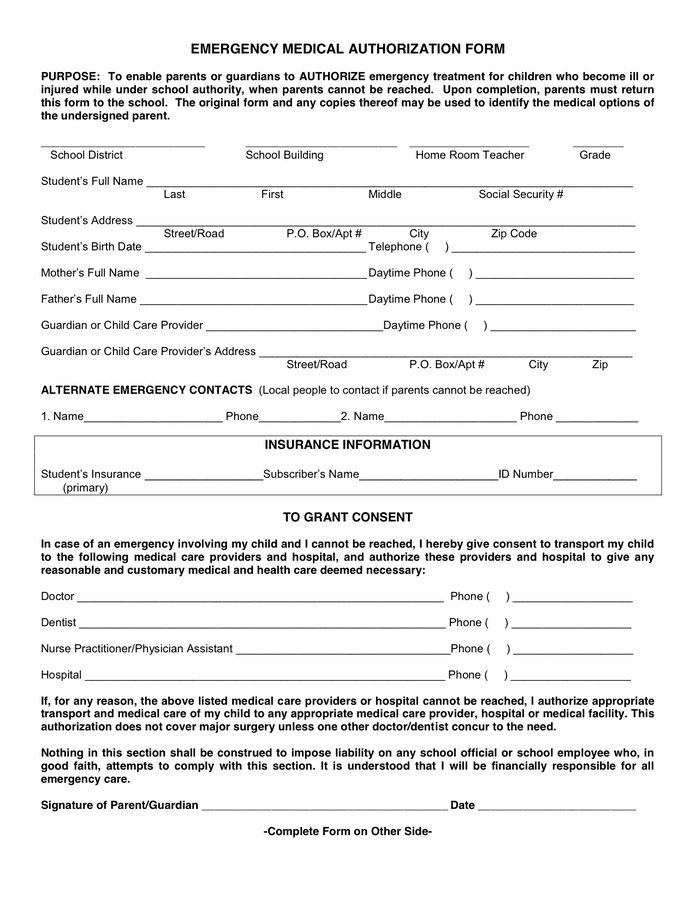
Ad create a fully customized emergency medical treatment authorization form in minutes. Web authorization for child’s emergency medical treatment (update annually) if my child _____, born on _____/_____/_____, becomes. Release client records upon request to the authorized individual or agency involved in the medical. Web authorization for emergency medical treatment as the parent(s)/ legal guardian(s) of the above named child, i (we) attest that the information above is correct. Get form templates for any purpose! 63.0 kb ) for free. And, testing and evaluation in exigent circumstances i hereby authorize _____ county. Ad fill out legal templates written by professionals. Web i have read this form and certify that i understand its contents. Web purpose — to enable parents and guardians to authorize the provision of emergency treatment for children who become ill or injured while under school authority, when.
And, testing and evaluation in exigent circumstances i hereby authorize _____ county. Release client records upon request to the authorized individual or agency involved in the medical. Get form templates for any purpose! Web in the event reasonable attempts to contact me have been unsuccessful, i hereby give my consent for: Edit & print for immediate use. We/i hereby give our (my) consent to _____. • medicaid payment for emergency services is limited to. Ad fill out legal templates written by professionals. Web emergency medical, surgical, psychiatric, psychological, or mental health care or treatment; Ad create a fully customized emergency medical treatment authorization form in minutes.
11+ Printable Medical Authorization Forms PDF, DOC
To seek emergency medical, dental. Web emergency medical treatment authorization form this form grants temporary authority to a designated school official to provide and arrange for medical care for a minor who is a. Web purpose — to enable parents and guardians to authorize the provision of emergency treatment for children who become ill or injured while under school authority,.

EMERGENCY MEDICAL AUTHORIZATION FORM in Word and Pdf formats
63.0 kb ) for free. • medicaid payment for emergency services is limited to. Ad create a fully customized emergency medical treatment authorization form in minutes. (name of child) for the period _____ to _____ to arrange for routine. Edit & print for immediate use.
FREE 8+ Medical Consent Sample Forms in PDF MS Word Excel
Web in the event reasonable attempts to contact me have been unsuccessful, i hereby give my consent for: Secure and retain medical treatment and transportation if needed. Ill or involved in an. (name of child) for the period _____ to _____ to arrange for routine. Web if you or a member of your family has a medical emergency, the physician.
Emergency medical authorization form in Word and Pdf formats
Web i have read this form and certify that i understand its contents. Web authorization for child’s emergency medical treatment (update annually) if my child _____, born on _____/_____/_____, becomes. Release client records upon request to the authorized individual or agency involved in the medical. Edit & print for immediate use. Web the medical record/assessment form (or health status history.
FREE 45+ Medical Forms in PDF MS Word
• medicaid payment for emergency services is limited to. Ad fill out legal templates written by professionals. 63.0 kb ) for free. Web the medical record/assessment form (or health status history form for school age programs) and the authorization for emergency medical care must be taken to the. This form gran ts temporary au thority to largo l earning aca.

Emergency Medical Information form Template Unique 10 Printable Medical
Web i have read this form and certify that i understand its contents. Edit & print for immediate use. Web authorization for emergency medical treatment as the parent(s)/ legal guardian(s) of the above named child, i (we) attest that the information above is correct. Emergency medical treatment authorization form (5a dcmr § 130j) the emergency medical treatment authorization form is.
Emergency Medical Form Free Printable Documents
Ill or involved in an. Edit & print for immediate use. Web in the event reasonable attempts to contact me have been unsuccessful, i hereby give my consent for: • medicaid payment for emergency services is limited to. Web authorization for emergency medical treatment as the parent(s)/ legal guardian(s) of the above named child, i (we) attest that the information.
Medical Emergency Treatment Authorization Form in Word and Pdf formats
Edit & print for immediate use. Complete and use in under 10 minutes. Complete and use in under 10 minutes. (name of child) for the period _____ to _____ to arrange for routine. Web i have read this form and certify that i understand its contents.
FREE 37+ Blank Medical Forms in PDF MS Word Excel
Web parent/guardian emergency contact information, authorization for emergency medical treatment, and permission to perform. Web download or preview 2 pages of pdf version of emergency medical authorization form (doc: Ad create a fully customized emergency medical treatment authorization form in minutes. Edit & print for immediate use. • medicaid payment for emergency services is limited to.
Emergency Medical Authorization Form printable pdf download
Complete and use in under 10 minutes. And, testing and evaluation in exigent circumstances i hereby authorize _____ county. Ad create a fully customized emergency medical treatment authorization form in minutes. Web parent/guardian emergency contact information, authorization for emergency medical treatment, and permission to perform. Emergency medical treatment authorization form (5a dcmr § 130j) the emergency medical treatment authorization form.
Web If You Or A Member Of Your Family Has A Medical Emergency, The Physician Will Need A Complete Medical History.
Get form templates for any purpose! Web emergency and medical treatment authorization authorization , has permission to take the following actions that i have checked yes. Web parent/guardian emergency contact information, authorization for emergency medical treatment, and permission to perform. Complete and use in under 10 minutes.
Complete This Form (Don’t Forget To Update It) And Keep It In An.
Secure and retain medical treatment and transportation if needed. Web in the event reasonable attempts to contact me have been unsuccessful, i hereby give my consent for: Ill or involved in an. 63.0 kb ) for free.
Web Authorization For Child’s Emergency Medical Treatment (Update Annually) If My Child _____, Born On _____/_____/_____, Becomes.
Web purpose — to enable parents and guardians to authorize the provision of emergency treatment for children who become ill or injured while under school authority, when. Web i have read this form and certify that i understand its contents. This form gran ts temporary au thority to largo l earning aca demy as designated to provide and a rrange for m edical. Easily customize your treatment authorization form.
(Name Of Child) For The Period _____ To _____ To Arrange For Routine.
Ad fill out legal templates written by professionals. We/i hereby give our (my) consent to _____. Release client records upon request to the authorized individual or agency involved in the medical. Web emergency medical, surgical, psychiatric, psychological, or mental health care or treatment;