Doh Form Pdf
Doh Form Pdf - Indicate n/a if an item does not apply to this patient or unk if the requested information is unknown to the physician signing this form. Web doh need a blank doh form? Applicant names list your name first. People have the right to get care from those they love and trust — people who bring them comfort & joy. Web cian's order is subject to the new york state department of health regulations at parts 515, 516, 517 and 518 of title 18 nycrr, which permit the department to impose monetary penalties on, or sanction and recover overpayments from, providers or prescribers of medical care, services or supplies when medical care, services or supplies that are For the condition(s) requiring personal care: Web americans with disabilities act complaint form (pdf) asbestos. Enter all relevant medical, mental health or physical conditions and/or limitations that impact the required mode of transportation for this enrollee in the box below. Include aliases and maiden name. Patient identifying information (use additional paper if necessary) 2.
Patient identifying information (use additional paper if necessary) 2. Indicate n/a if an item does not apply to this patient or unk if the requested information is unknown to the physician signing this form. Applicant names list your name first. This form also outlines what, and with whom, health information can be shared. *[please note, children less than 18 years of age who are parents, pregnant, and/or married, and who are otherwise capable of consenting, should not use this form. People have the right to get care from those they love and trust — people who bring them comfort & joy. Web this form must be used for children less than 18 years of age for enrollment in a health home. • age 65 or older • certified blind or certified disabled (of any age) • not certified disabled but chronically ill • institutionalized and applying for coverage of nursing home care. Web cian's order is subject to the new york state department of health regulations at parts 515, 516, 517 and 518 of title 18 nycrr, which permit the department to impose monetary penalties on, or sanction and recover overpayments from, providers or prescribers of medical care, services or supplies when medical care, services or supplies that are For the condition(s) requiring personal care:
Applicant names list your name first. *[please note, children less than 18 years of age who are parents, pregnant, and/or married, and who are otherwise capable of consenting, should not use this form. People have the right to get care from those they love and trust — people who bring them comfort & joy. Include aliases and maiden name. Web americans with disabilities act complaint form (pdf) asbestos. • age 65 or older • certified blind or certified disabled (of any age) • not certified disabled but chronically ill • institutionalized and applying for coverage of nursing home care. Patient identifying information (use additional paper if necessary) 2. This form also outlines what, and with whom, health information can be shared. Web doh need a blank doh form? Enter all relevant medical, mental health or physical conditions and/or limitations that impact the required mode of transportation for this enrollee in the box below.

Doh Form 116m Fill Online, Printable, Fillable, Blank PDFfiller
Web doh need a blank doh form? Include aliases and maiden name. Enter all relevant medical, mental health or physical conditions and/or limitations that impact the required mode of transportation for this enrollee in the box below. Web this form must be used for children less than 18 years of age for enrollment in a health home. People have the.
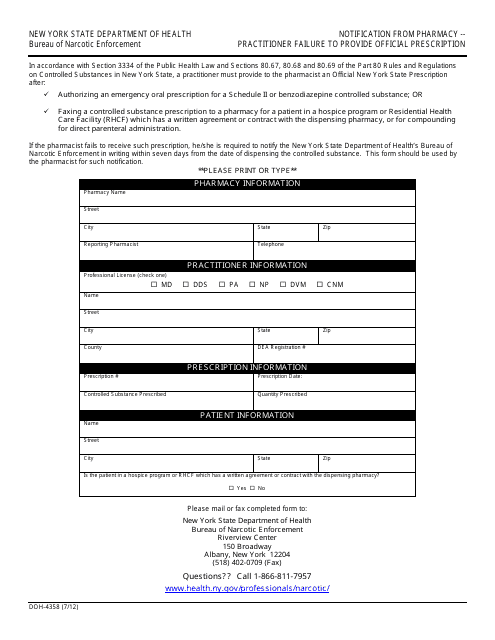
Form DOH4358 Download Printable PDF or Fill Online Notification From
If necessary, attach an extra sheet to list all children. For the condition(s) requiring personal care: Patient identifying information (use additional paper if necessary) 2. Include aliases and maiden name. Enter all relevant medical, mental health or physical conditions and/or limitations that impact the required mode of transportation for this enrollee in the box below.
Doh Form Fill Out and Sign Printable PDF Template signNow
Applicant names list your name first. • age 65 or older • certified blind or certified disabled (of any age) • not certified disabled but chronically ill • institutionalized and applying for coverage of nursing home care. Include aliases and maiden name. If necessary, attach an extra sheet to list all children. People have the right to get care from.
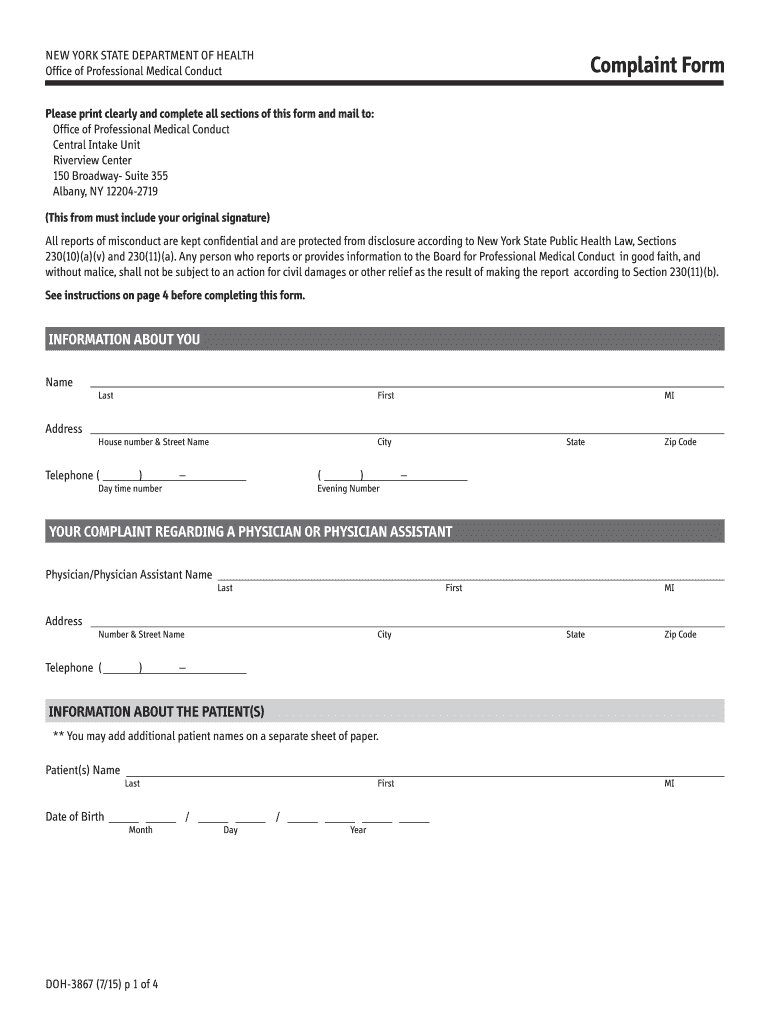
20152021 Form NY DOH3867 Fill Online, Printable, Fillable, Blank
Web doh need a blank doh form? Enter all relevant medical, mental health or physical conditions and/or limitations that impact the required mode of transportation for this enrollee in the box below. Applicant names list your name first. Web americans with disabilities act complaint form (pdf) asbestos. *[please note, children less than 18 years of age who are parents, pregnant,.

Doh 4359 form Fill out & sign online DocHub
Include aliases and maiden name. Web americans with disabilities act complaint form (pdf) asbestos. People have the right to get care from those they love and trust — people who bring them comfort & joy. Web cian's order is subject to the new york state department of health regulations at parts 515, 516, 517 and 518 of title 18 nycrr,.
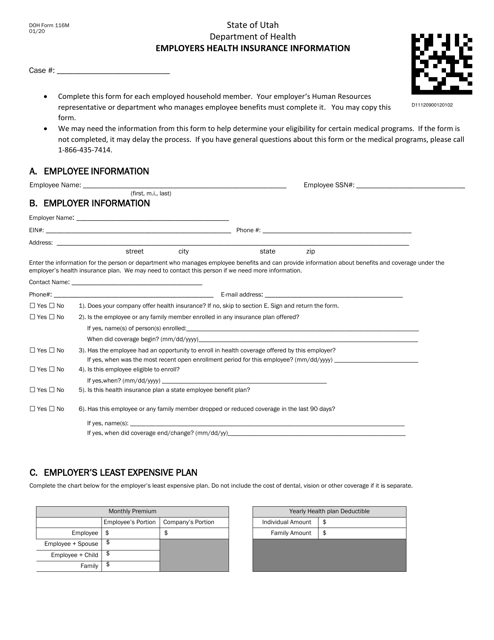
DOH Form 116M Download Printable PDF or Fill Online Employers Health
Include aliases and maiden name. Patient identifying information (use additional paper if necessary) 2. People have the right to get care from those they love and trust — people who bring them comfort & joy. For the condition(s) requiring personal care: Indicate n/a if an item does not apply to this patient or unk if the requested information is unknown.
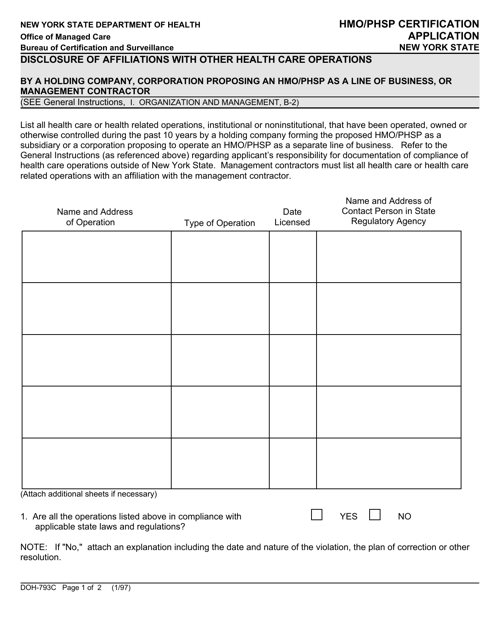
Form DOH793C Download Printable PDF or Fill Online HMO/Phsp
Web doh need a blank doh form? Web this form must be used for children less than 18 years of age for enrollment in a health home. This form also outlines what, and with whom, health information can be shared. Patient identifying information (use additional paper if necessary) 2. If necessary, attach an extra sheet to list all children.
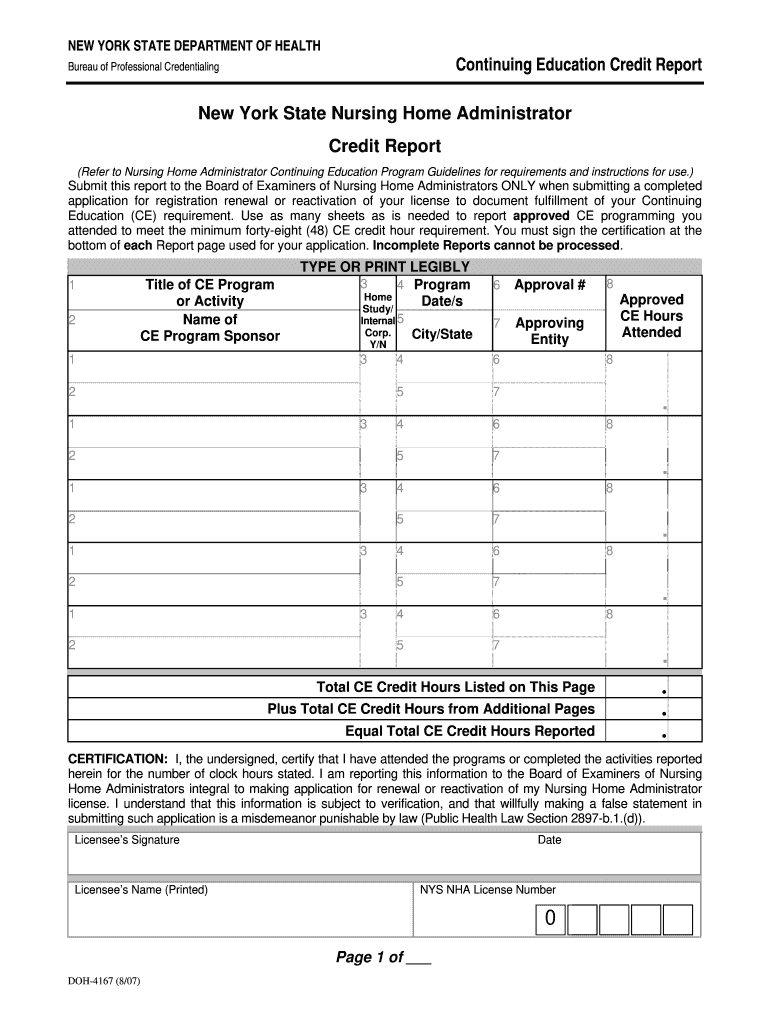
Doh 4167 Fill Online, Printable, Fillable, Blank pdfFiller
Web cian's order is subject to the new york state department of health regulations at parts 515, 516, 517 and 518 of title 18 nycrr, which permit the department to impose monetary penalties on, or sanction and recover overpayments from, providers or prescribers of medical care, services or supplies when medical care, services or supplies that are Web doh need.
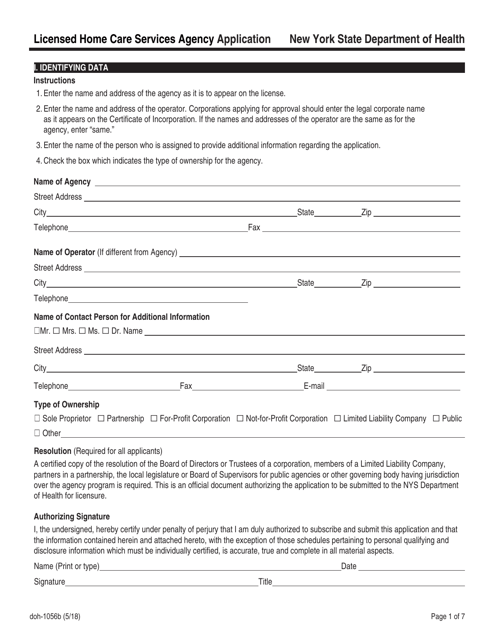
Form DOH1056B Download Fillable PDF or Fill Online Licensed Home Care
Enter all relevant medical, mental health or physical conditions and/or limitations that impact the required mode of transportation for this enrollee in the box below. *[please note, children less than 18 years of age who are parents, pregnant, and/or married, and who are otherwise capable of consenting, should not use this form. People have the right to get care from.
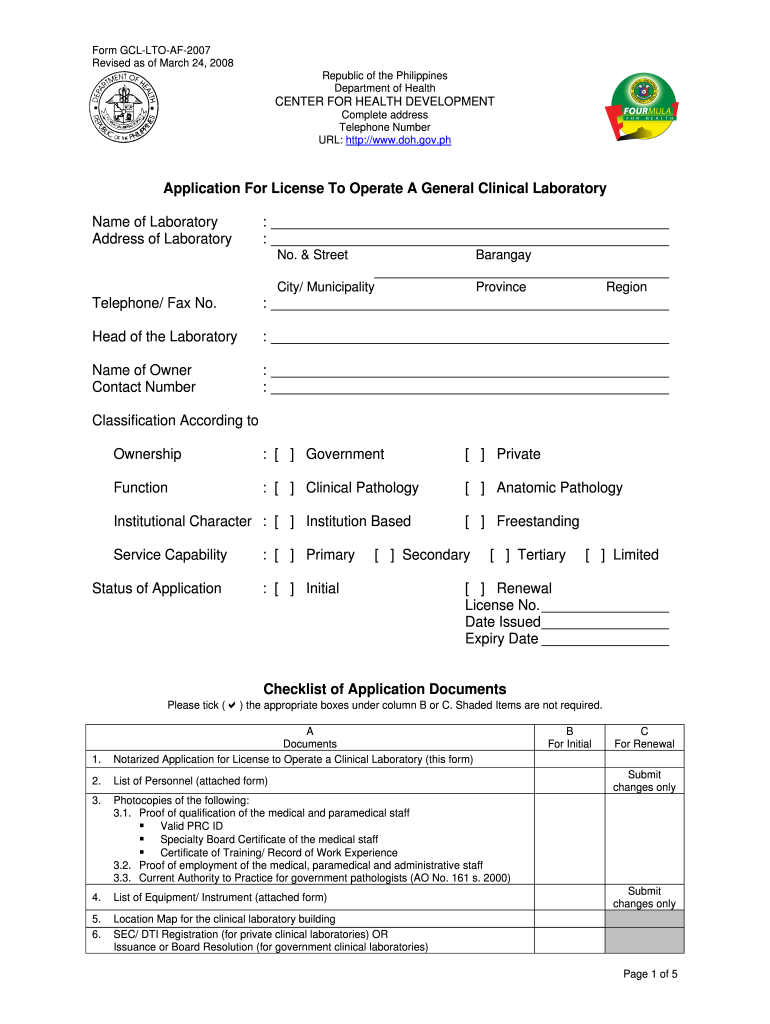
Doh Application Form for Renewal of License to Operate Fill Out and
Enter all relevant medical, mental health or physical conditions and/or limitations that impact the required mode of transportation for this enrollee in the box below. *[please note, children less than 18 years of age who are parents, pregnant, and/or married, and who are otherwise capable of consenting, should not use this form. Include aliases and maiden name. • age 65.
This Form Also Outlines What, And With Whom, Health Information Can Be Shared.
*[please note, children less than 18 years of age who are parents, pregnant, and/or married, and who are otherwise capable of consenting, should not use this form. If necessary, attach an extra sheet to list all children. Indicate n/a if an item does not apply to this patient or unk if the requested information is unknown to the physician signing this form. For the condition(s) requiring personal care:
Web This Form Must Be Used For Children Less Than 18 Years Of Age For Enrollment In A Health Home.
Enter all relevant medical, mental health or physical conditions and/or limitations that impact the required mode of transportation for this enrollee in the box below. • age 65 or older • certified blind or certified disabled (of any age) • not certified disabled but chronically ill • institutionalized and applying for coverage of nursing home care. Patient identifying information (use additional paper if necessary) 2. Web americans with disabilities act complaint form (pdf) asbestos.
Web Cian's Order Is Subject To The New York State Department Of Health Regulations At Parts 515, 516, 517 And 518 Of Title 18 Nycrr, Which Permit The Department To Impose Monetary Penalties On, Or Sanction And Recover Overpayments From, Providers Or Prescribers Of Medical Care, Services Or Supplies When Medical Care, Services Or Supplies That Are
People have the right to get care from those they love and trust — people who bring them comfort & joy. Include aliases and maiden name. Web doh need a blank doh form? Applicant names list your name first.