Dental Health History Form Pdf
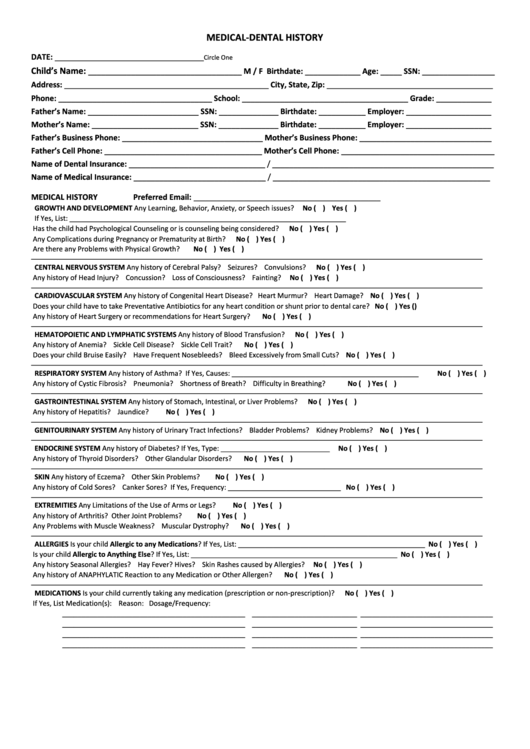
Dental Health History Form Pdf - Web health history form email: The form is available in a digital, downloadable version or in print. Includ es questions related to dental history, medications and other substances, allergies. Web dental health history form. Web medical and dental health history form getting to know you as our patient account number: Web health history form dental information for the following questions, please mark (x) your responses to the following questions. Once the medical/dental health history form is completed, the dentist should: It can be completed prior to or at the beginning of the initial appointment. As required by law, our office adheres to written policies and procedures to protect the privacy of information about you that we create, receive or maintain. _____________________ when was your last cleaning?
Web please complete both sides of this dental/medical history form so that we may provide you with the best possible dental care. Includ es questions related to dental history, medications and other substances, allergies. Date of last dental examination: Why have you come to see us. I acknowledge that my questions, if any, about inquiries set forth. As required by law, our office adheres to written policies and procedures to protect the privacy of information about you that we create, receive or maintain. It can be completed prior to or at the beginning of the initial appointment. Web health history form dental information for the following questions, please mark (x) your responses to the following questions. Web medical and dental health history form getting to know you as our patient account number: Web sample health history forms are available through the american dental association’s (ada) department of product development and sales and can be ordered online.
Why have you come to see us. The document is available in both english and spanish; Web use the 2021 edition of the ada patient dental and medical health history information form to collect pertinent health information and history from your patients before treatment. Includ es questions related to dental history, medications and other substances, allergies. Web health history form email: Web please complete both sides of this dental/medical history form so that we may provide you with the best possible dental care. What is the reason for your visit today? Different forms are available for children and adults. The form is available in a digital, downloadable version or in print. Patient name (?rst and last):
Patient Medical And Dental History Form printable pdf download
Different forms are available for children and adults. Why have you come to see us. Web please complete both sides of this dental/medical history form so that we may provide you with the best possible dental care. Web sample health history forms are available through the american dental association’s (ada) department of product development and sales and can be ordered.
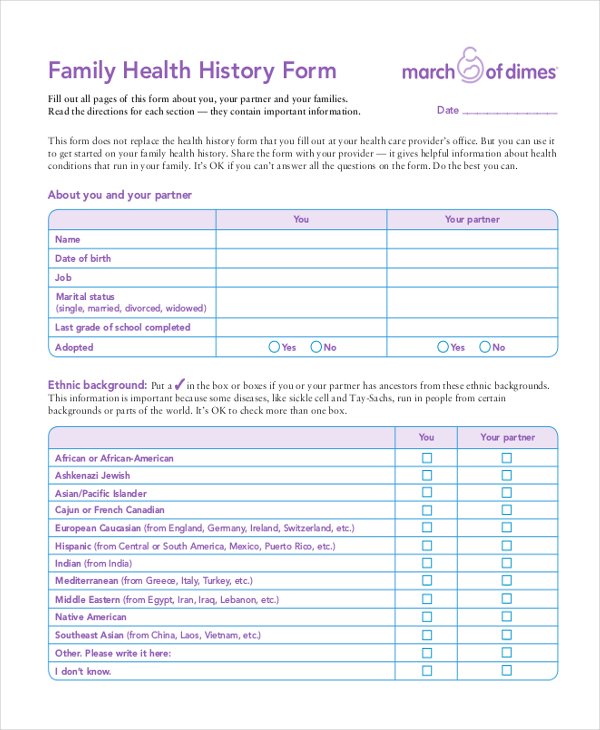
![43 Medical Health History Forms [PDF, Word] ᐅ TemplateLab](https://templatelab.com/wp-content/uploads/2021/02/health-history-form-03-scaled-e1617709269345.jpg)
43 Medical Health History Forms [PDF, Word] ᐅ TemplateLab
Includ es questions related to dental history, medications and other substances, allergies. The form is available in a digital, downloadable version or in print. Web the american dental association (ada) offers a comprehensive health history form, for adults or children in both english and spanish, that covers both medical and dental issues. Your answers are for our records only and.
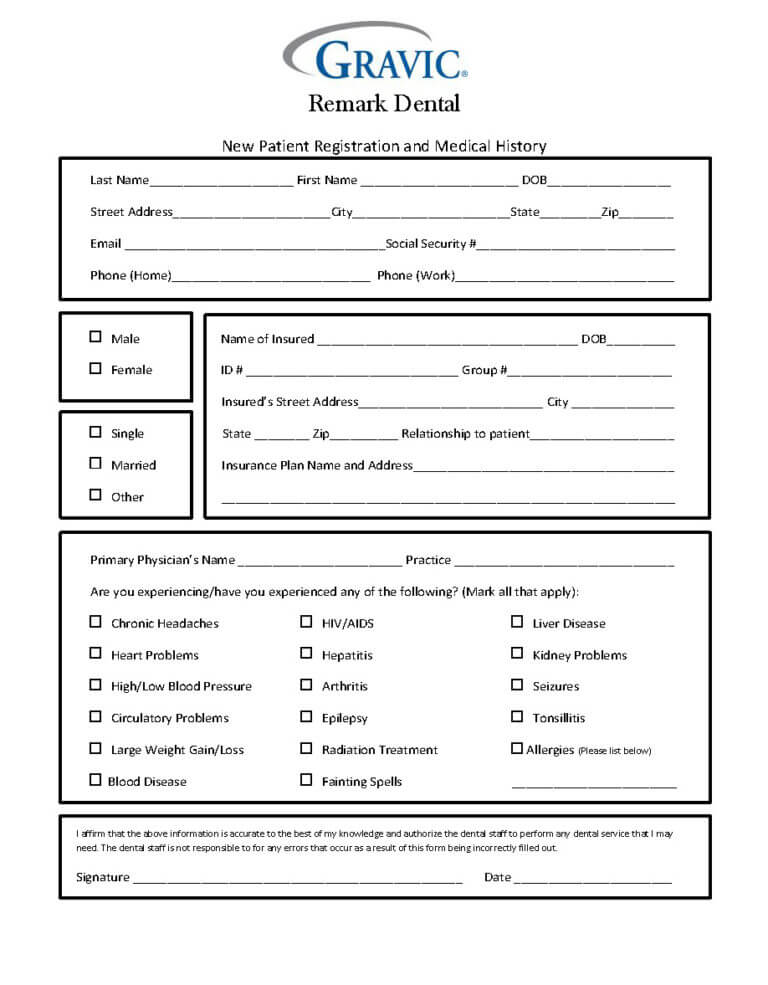
Dental Patient History Form · Remark Software With Regard To Medical
What is the reason for your visit today? Different forms are available for children and adults. Web health history form dental information for the following questions, please mark (x) your responses to the following questions. Why have you come to see us. Web health history form email:
FREE 12+ Sample Health History Forms in PDF Excel Word
Web sample health history forms are available through the american dental association’s (ada) department of product development and sales and can be ordered online. I understand the importance of a truthful health history and that my dentist and his/her staff will rely on this information for treating me. Patient name (?rst and last): Web the american dental association (ada) offers.
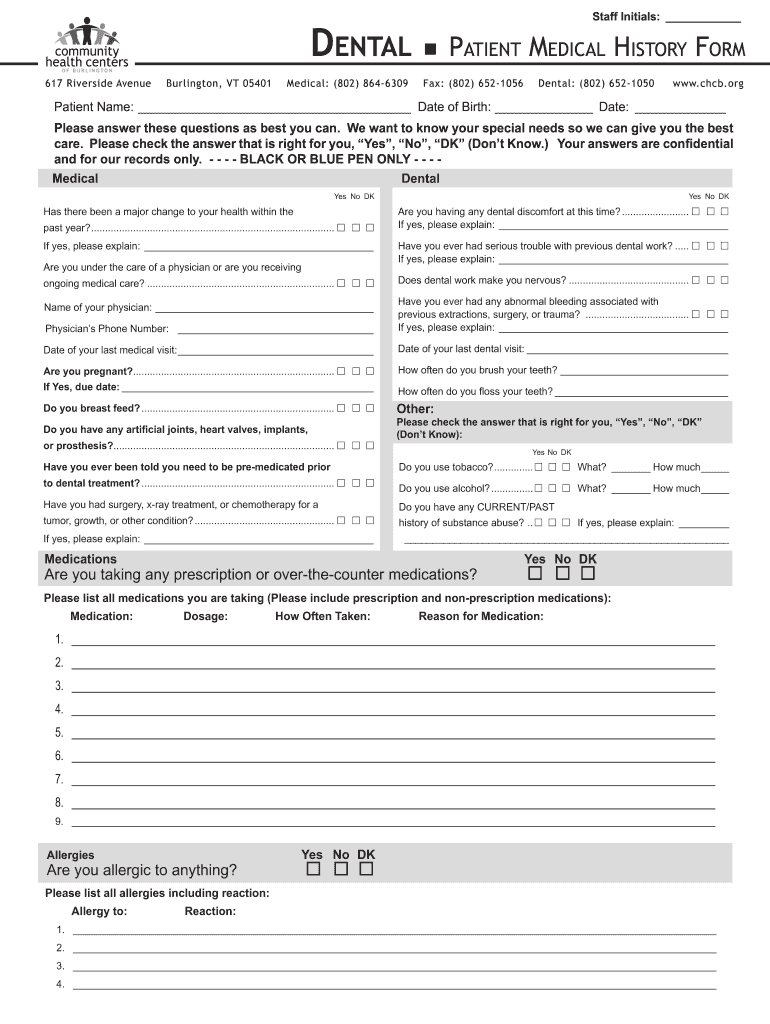
Dental Patient Medical Form Fill Online, Printable, Fillable, Blank
_____________________ when was your last cleaning? The document is available in both english and spanish; Includ es questions related to dental history, medications and other substances, allergies. Web health history form email: Web the american dental association (ada) offers a comprehensive health history form, for adults or children in both english and spanish, that covers both medical and dental issues.
FREE 12+ Sample Health History Forms in PDF Excel Word
Web (over please) rev 6/2018 adult medical and dental history dental history former dentist _____________________________________ address_______________________________________ when did you last visit a dentist? Why have you come to see us. The form is available in a digital, downloadable version or in print. It can be completed prior to or at the beginning of the initial appointment. The document is available.
FREE 23+ Sample Medical History Forms in PDF Word Excel
Web health history form email: Your answers are for our records only and will be kept confidential subject to applicable laws. Date of last dental examination: The document is available in both english and spanish; Web sample health history forms are available through the american dental association’s (ada) department of product development and sales and can be ordered online.
Dental History Form printable pdf download
Date of last dental examination: All information is completely confidential. Web health history form email: Web please complete both sides of this dental/medical history form so that we may provide you with the best possible dental care. Web health history form dental information for the following questions, please mark (x) your responses to the following questions.
FREE 43+ Sample Medical Forms in PDF
Web sample health history forms are available through the american dental association’s (ada) department of product development and sales and can be ordered online. Web dental health history form. The document is available in both english and spanish; The form is available in a digital, downloadable version or in print. As required by law, our office adheres to written policies.
Dental Health History Form printable pdf download
I acknowledge that my questions, if any, about inquiries set forth. Why have you come to see us. Web use the 2021 edition of the ada patient dental and medical health history information form to collect pertinent health information and history from your patients before treatment. Patient name (?rst and last): As required by law, our office adheres to written.
Once The Medical/Dental Health History Form Is Completed, The Dentist Should:
Your answers are for our records only and will be kept confidential subject to applicable laws. Web the american dental association (ada) offers a comprehensive health history form, for adults or children in both english and spanish, that covers both medical and dental issues. Date of last dental examination: It can be completed prior to or at the beginning of the initial appointment.
Web Dental Health History Form.
The form is available in a digital, downloadable version or in print. All information is completely confidential. _____________________ when was your last cleaning? Web medical and dental health history form getting to know you as our patient account number:
As Required By Law, Our Office Adheres To Written Policies And Procedures To Protect The Privacy Of Information About You That We Create, Receive Or Maintain.
Web health history form dental information for the following questions, please mark (x) your responses to the following questions. Includ es questions related to dental history, medications and other substances, allergies. Patient name (?rst and last): Web (over please) rev 6/2018 adult medical and dental history dental history former dentist _____________________________________ address_______________________________________ when did you last visit a dentist?
The Document Is Available In Both English And Spanish;
What is the reason for your visit today? I acknowledge that my questions, if any, about inquiries set forth. Why have you come to see us. Web please complete both sides of this dental/medical history form so that we may provide you with the best possible dental care.