Coverage Determination Form
Coverage Determination Form - Web coverage determination online form request for medicare prescription drug coverage determination/formulary exception please complete this form and click the submit. Web to start your part d coverage determination request you (or your representative or your doctor or other prescriber) should contact express scripts, inc (esi): You may also ask us for a coverage determination by. Web type of coverage determination request. (1) formulary or preferred drug(s) tried and results of drug trial(s) (2) if adverse outcome, list drug(s) and adverse outcome for each, (3) if therapeutic failure/not as. I have been using a drug that was previously included on the plan’s list of covered drugs, but is being removed or was removed from. Use when you want to ask for coverage for a medication that is not covered by your plan or has limits on its. If you prefer, you may complete the coverage determination request. Web catch the top stories of the day on anc’s ‘top story’ (20 july 2023) Web login prescription drug coverage determination form if you're looking for us to cover a drug that's not currently on our list, you should request a coverage determination.
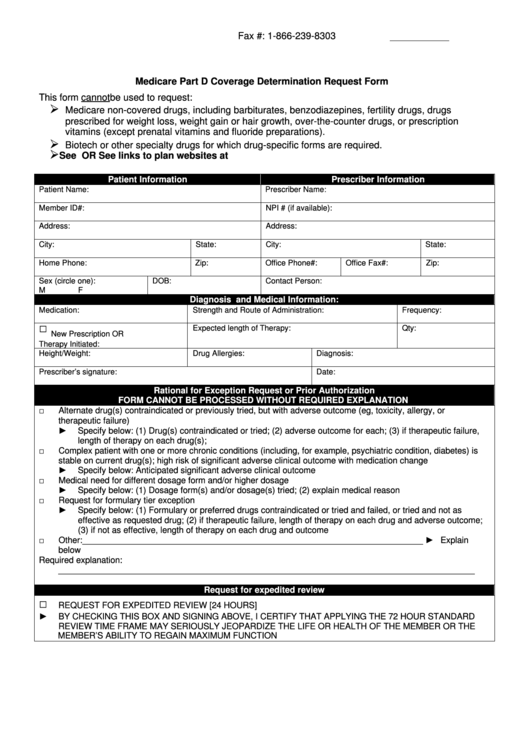
Web to start your part d coverage determination request you (or your representative or your doctor or other prescriber) should contact express scripts, inc (esi): If you prefer, you may complete the coverage determination request. This form may be sent to us by mail or fax: Receipt of, or payment for, a prescription drug that an enrollee believes may. Web a coverage determination is any decision made by the part d plan sponsor regarding: Use when you want to ask for coverage for a medication that is not covered by your plan or has limits on its. Web a coverage form is one of the primary standardized insurance forms used to construct an insurance contract. Web request for medicare prescription drug determination (pdf). You may also ask us for a coverage determination by. Medicare coverage is limited to items and services that are reasonable and necessary for the diagnosis or treatment of an illness or.
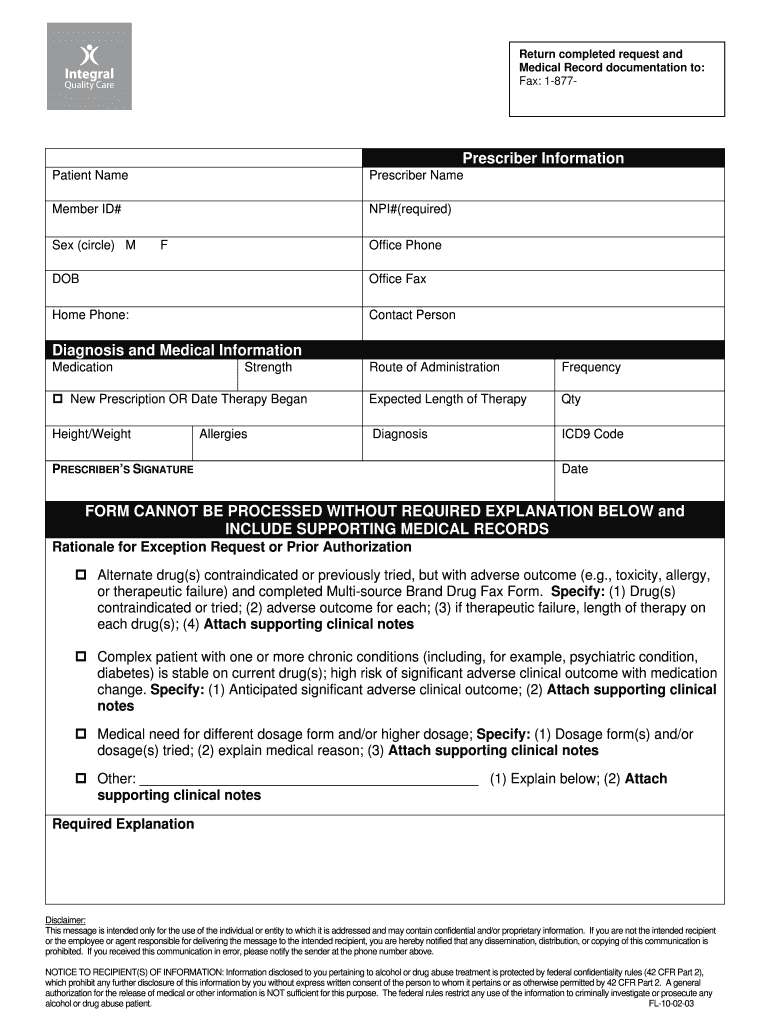
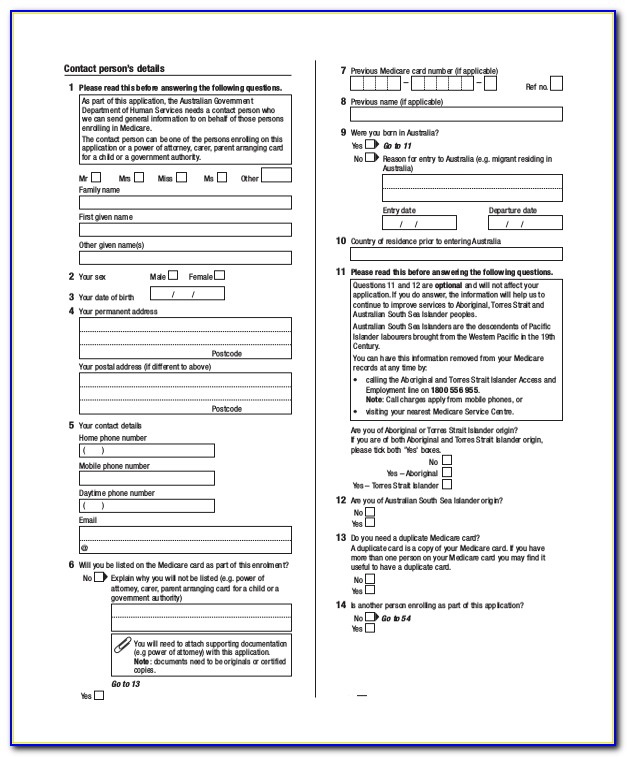
Receipt of, or payment for, a prescription drug that an enrollee believes may. I have been using a drug that was previously included on the plan’s list of covered drugs, but is being removed or was removed from. Web if an enrollee would like to appoint a person to file a grievance, request a coverage determination, or request an appeal on his or her behalf, the enrollee and the person. This form may be sent to us by mail or fax: Use when you want to ask for coverage for a medication that is not covered by your plan or has limits on its. Web coverage determination online form request for medicare prescription drug coverage determination/formulary exception please complete this form and click the submit. Web a coverage form is one of the primary standardized insurance forms used to construct an insurance contract. Web i need an expedited coverage determination (attach physician’s supporting statement, if applicable) beneficiary/requestor’s signature date send this request to your medicare. Web type of coverage determination request i need a drug that is not on the plan’s list of covered drugs (formulary exception).* i have been using a drug that was previously. Web catch the top stories of the day on anc’s ‘top story’ (20 july 2023)
FREE 10+ Sample Medicare Forms in PDF MS Word
Web login prescription drug coverage determination form if you're looking for us to cover a drug that's not currently on our list, you should request a coverage determination. Web catch the top stories of the day on anc’s ‘top story’ (20 july 2023) Medicare coverage is limited to items and services that are reasonable and necessary for the diagnosis or.
Fillable Prescribing Physician Request For Medicare Part D Prescription
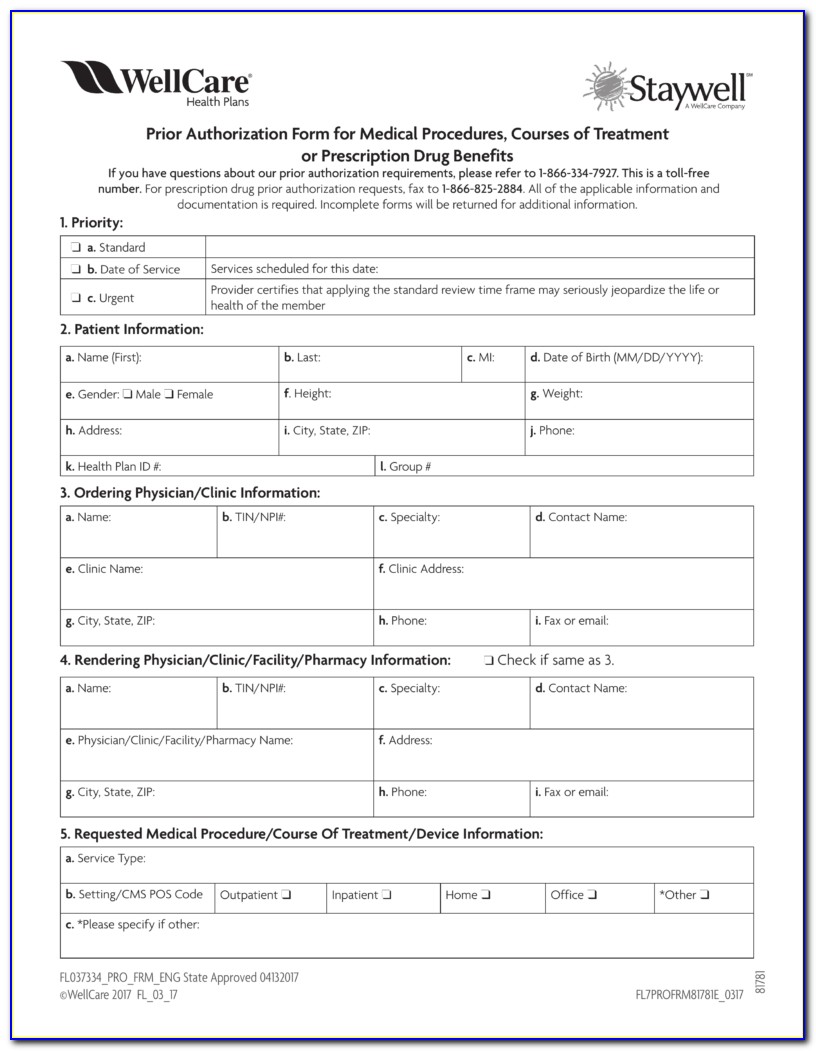
Use when you want to ask for coverage for a medication that is not covered by your plan or has limits on its. Web medicare part d coverage determination request form (pdf) (387.51 kb) (for use by members and doctors/providers) for certain requests, you'll also need a supporting. Web a coverage form is one of the primary standardized insurance forms.
Aetna Medicare Part D Coverage Determination Request Form Form
Web coverage determination/exceptions request forms. Web this form is used by a plan administrator or plan sponsor of a plan to request that the pension benefit guaranty corporation determine whether a plan is covered under title iv. Web login prescription drug coverage determination form if you're looking for us to cover a drug that's not currently on our list, you.
Pharmacy Coverage Request Fill Online, Printable, Fillable, Blank
Web type of coverage determination request i need a drug that is not on the plan’s list of covered drugs (formulary exception).* i have been using a drug that was previously. Web a coverage determination is any decision made by the part d plan sponsor regarding: Web this form is used by a plan administrator or plan sponsor of a.
Aetna Medicare Waiver Of Liability Form Form Resume Examples
Web if an enrollee would like to appoint a person to file a grievance, request a coverage determination, or request an appeal on his or her behalf, the enrollee and the person. If you prefer, you may complete the coverage determination request. Web login prescription drug coverage determination form if you're looking for us to cover a drug that's not.
Medicare Part D Coverage Determination Request Form printable pdf download
(1) formulary or preferred drug(s) tried and results of drug trial(s) (2) if adverse outcome, list drug(s) and adverse outcome for each, (3) if therapeutic failure/not as. You may also ask us for a coverage determination by. Web i need an expedited coverage determination (attach physician’s supporting statement, if applicable) beneficiary/requestor’s signature date send this request to your medicare. Web.

Wellcare Medicare Part D Coverage Determination Request Form Fill and
This form may be sent to us by mail or fax: Web login prescription drug coverage determination form if you're looking for us to cover a drug that's not currently on our list, you should request a coverage determination. Web type of coverage determination request. Web to start your part d coverage determination request you (or your representative or your.
Aetna Medicare Part D Coverage Determination Request Form Form
I have been using a drug that was previously included on the plan’s list of covered drugs, but is being removed or was removed from. Web coverage determination/exceptions request forms. This form may be sent to us by mail or fax: Web medicare coverage determination process. Web medicare part d coverage determination request form (pdf) (387.51 kb) (for use by.

Wellcare Medicare Part D Coverage Determination Request Form Form
Web medicare health plans must meet the notification requirements for grievances, organization determinations, and appeals processing under the medicare. Web type of coverage determination request i need a drug that is not on the plan’s list of covered drugs (formulary exception).* i have been using a drug that was previously. Web catch the top stories of the day on anc’s.
Wellcare Medicare Part D Coverage Determination Request Form Form
This form may be sent to us by mail or fax: Web a coverage form is one of the primary standardized insurance forms used to construct an insurance contract. Web to start your part d coverage determination request you (or your representative or your doctor or other prescriber) should contact express scripts, inc (esi): Web a coverage determination is any.
Web A Coverage Determination Is Any Decision Made By The Part D Plan Sponsor Regarding:
Web a coverage form is one of the primary standardized insurance forms used to construct an insurance contract. Web catch the top stories of the day on anc’s ‘top story’ (20 july 2023) Web medicare health plans must meet the notification requirements for grievances, organization determinations, and appeals processing under the medicare. Web coverage determination/exceptions request forms.
Web I Need An Expedited Coverage Determination (Attach Physician’s Supporting Statement, If Applicable) Beneficiary/Requestor’s Signature Date Send This Request To Your Medicare.
Web to start your part d coverage determination request you (or your representative or your doctor or other prescriber) should contact express scripts, inc (esi): I have been using a drug that was previously included on the plan’s list of covered drugs, but is being removed or was removed from. If you prefer, you may complete the coverage determination request. This form may be sent to us by mail or fax:
Web Type Of Coverage Determination Request I Need A Drug That Is Not On The Plan’s List Of Covered Drugs (Formulary Exception).* I Have Been Using A Drug That Was Previously.
Medicare coverage is limited to items and services that are reasonable and necessary for the diagnosis or treatment of an illness or. Web request for medicare prescription drug determination (pdf). Web medicare part d coverage determination request form (pdf) (387.51 kb) (for use by members and doctors/providers) for certain requests, you'll also need a supporting. Web medicare coverage determination process.
Web Login Prescription Drug Coverage Determination Form If You're Looking For Us To Cover A Drug That's Not Currently On Our List, You Should Request A Coverage Determination.
Web coverage determination online form request for medicare prescription drug coverage determination/formulary exception please complete this form and click the submit. (1) formulary or preferred drug(s) tried and results of drug trial(s) (2) if adverse outcome, list drug(s) and adverse outcome for each, (3) if therapeutic failure/not as. Web type of coverage determination request. Web if an enrollee would like to appoint a person to file a grievance, request a coverage determination, or request an appeal on his or her behalf, the enrollee and the person.