Completed Cms 1500 Form
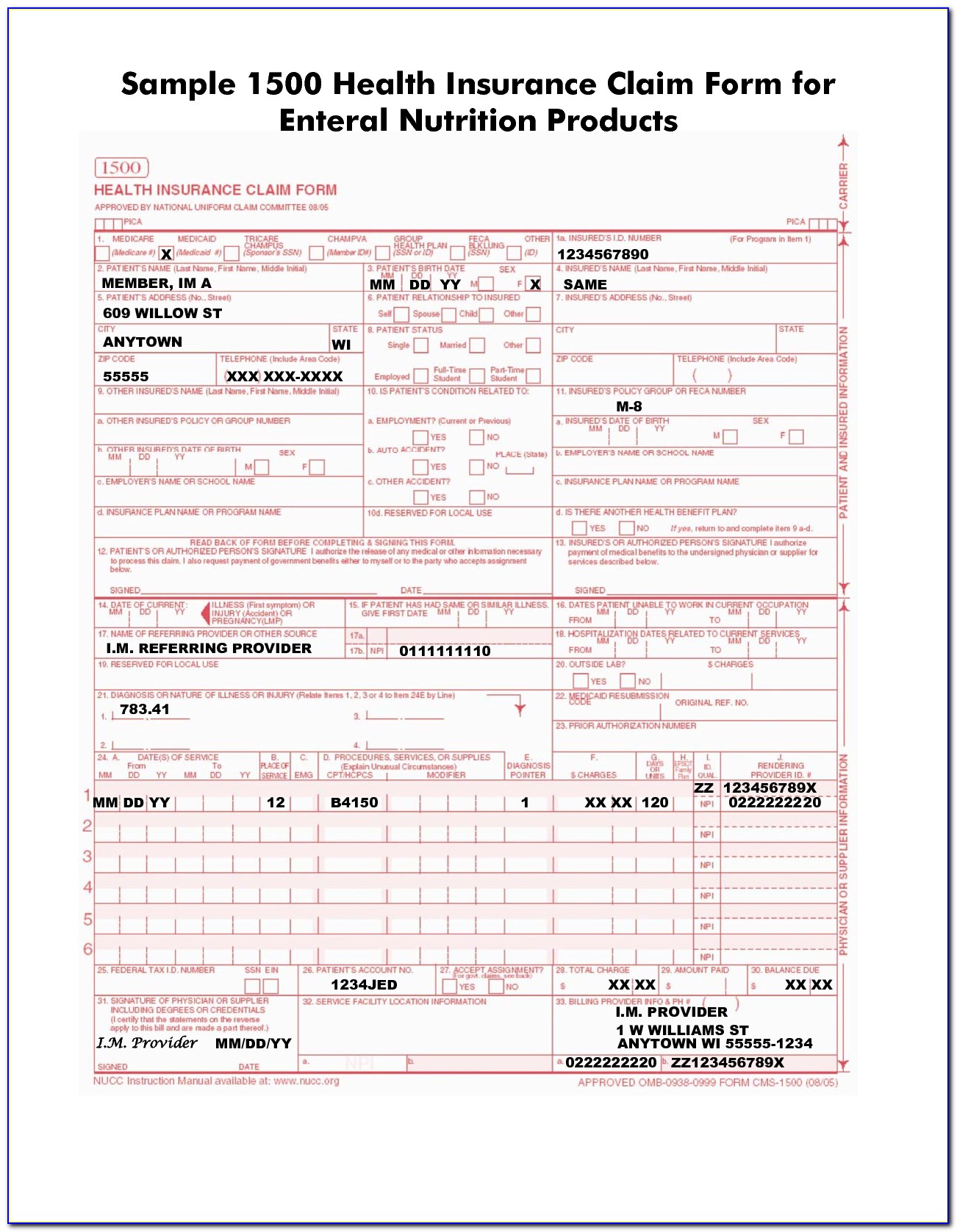
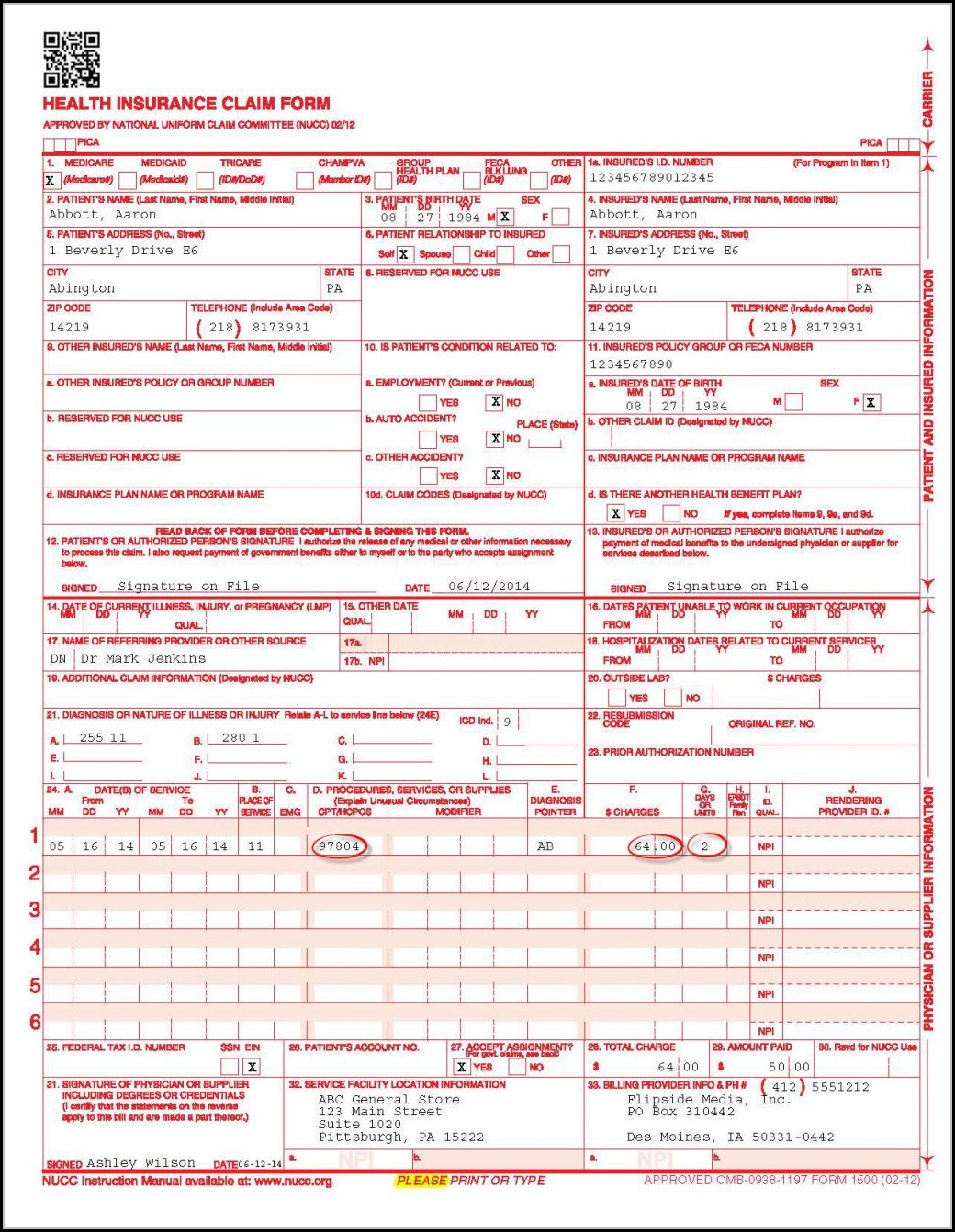
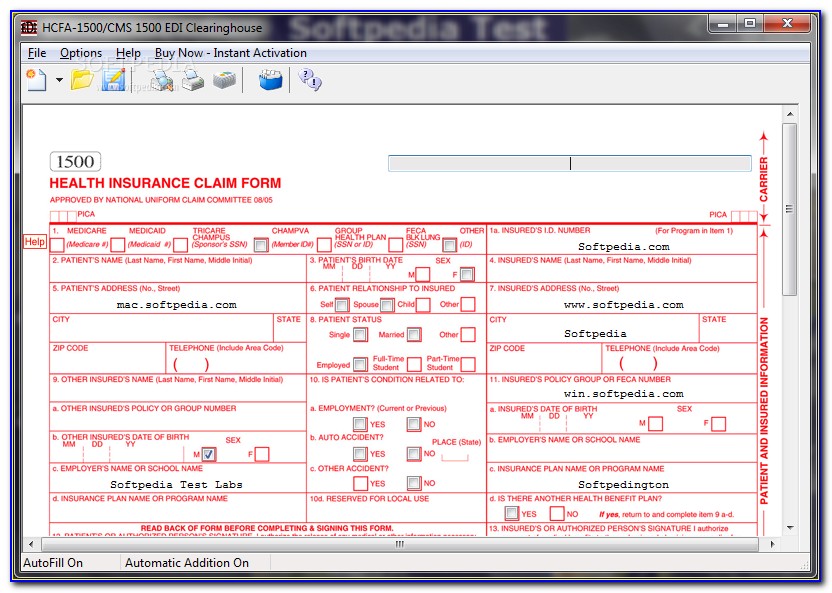
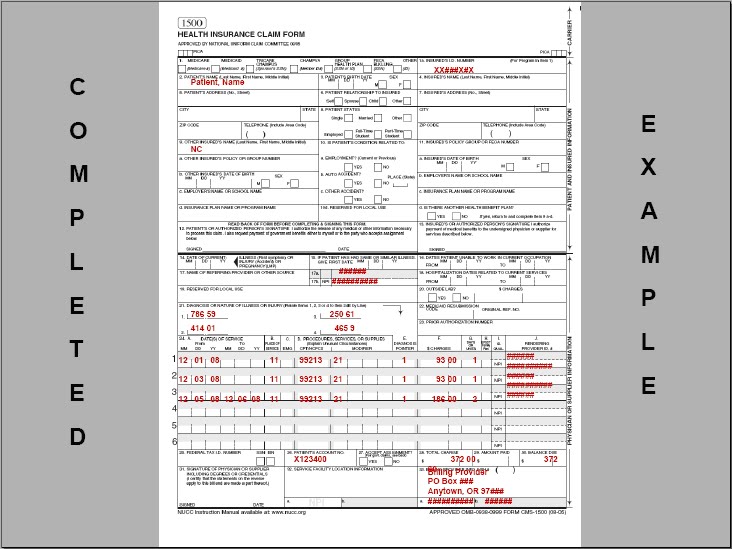
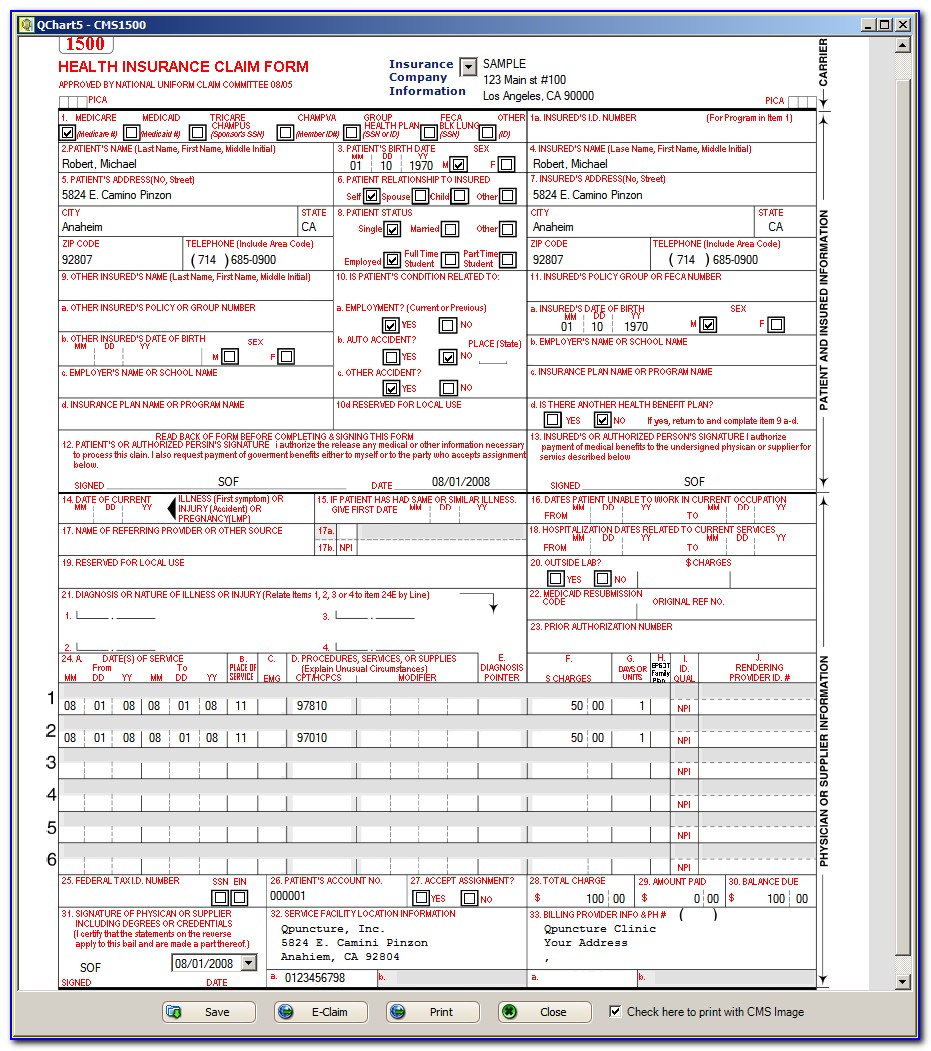
Completed Cms 1500 Form - Write down the patient's full name, birth date, sex, and address. To ensure timely processing of the claim form, you must follow the form instructions and complete all required information. Enter the insured's full name, address, and the patient's relationship to the. Insured’s address (no., street) city state zip code telephone (include area code) 11. The center of medicaid and medicare services (cms) form 1500 is used to bill sfhp for medical services. Insured’s policy group or feca number a. Claims may be electronically submitted to a medicare carrier, durable medical equipment medicare administrative contractor (dmemac), or a/b mac from a provider's office using a computer with software that meets electronic filing requirements as established by the hipaa claim. You can decide how often to. Web cms 1500 dynamic list information. And o veterans benefits (type 42).
Sign up to get the latest information about your choice of cms topics. This form is maintained by the national uniform claim committee (nucc), an industry organization in which cms participates. Web the center of medicaid and medicare services (cms) form 1500 must be used to bill sfhp for medical services. You can decide how often to. Web the 1500 health insurance claim form (1500 claim form) is in the public domain. Enter the insured's full name, address, and the patient's relationship to the. O black lung (type 41); This is the only format that is accepted. You'll see instructions on how to complete the field. The form is used by physicians and allied health professionals to submit claims for medical services.
The center of medicaid and medicare services (cms) form 1500 is used to bill sfhp for medical services. Sign up to get the latest information about your choice of cms topics. All paper claims you submit must be on the appropriate cms claim form. Failure to properly complete mandatory requirements will cause the claim to be denied by south dakota (sd) medicaid. Insured’s address (no., street) city state zip code telephone (include area code) 11. Insured’s name (last name, first name, middle initial) 7. The nucc has developed this general instructions document for completing the 1500claim form. Enter the insured's full name, address, and the patient's relationship to the. Web the 1500 health insurance claim form (1500 claim form) is in the public domain. This is the only format that is accepted.
Completed Cms 1500 Claim Form Sample Form Resume Examples K75PBGVkl2
Failure to properly complete mandatory requirements will cause the claim to be denied by south dakota (sd) medicaid. O black lung (type 41); Enter the insured's full name, address, and the patient's relationship to the. Failure to follow these guidelines could cause a delay in processing, denial of the claim, or affect payment accuracy. This form is maintained by the.

Completed Cms 1500 Form Sample Form Resume Examples 9x8raJV3dR
The nucc has developed this general instructions document for completing the 1500claim form. The cms claim form is available in red ink. Write down the patient's full name, birth date, sex, and address. Last updated wed, 04 jan 2023 13:36:02 +0000. Failure to properly complete mandatory requirements will cause the claim to be denied by south dakota (sd) medicaid.

Completed Cms 1500 Form Sample Form Resume Examples 9x8raJV3dR
Sign up to get the latest information about your choice of cms topics. Failure to follow these guidelines could cause a delay in processing, denial of the claim, or affect payment accuracy. State the type of health insurance applicable to this claim and the insured's id number; Web the center of medicaid and medicare services (cms) form 1500 must be.

Completed Cms 1500 Form Sample Form Resume Examples 9x8raJV3dR
Number (for program in item 1) 4. It can be purchased in any version required by calling the u.s. Web cms 1500 form o workers’ compensation (type 15); The form is used by physicians and allied health professionals to submit claims for medical services. Claims may be electronically submitted to a medicare carrier, durable medical equipment medicare administrative contractor (dmemac),.
Completed Cms 1500 Form Sample Form Resume Examples 9x8raJV3dR
All items must be completed unless otherwise noted in these instructions. This form is the only version accepted by medicare. The center of medicaid and medicare services (cms) form 1500 is used to bill sfhp for medical services. This is the only format that is accepted. Failure to properly complete mandatory requirements will cause the claim to be denied by.

Form Cms 1500 Instructions Form Resume Examples Wk9y1XX93D
Last updated wed, 04 jan 2023 13:36:02 +0000. All paper claims you submit must be on the appropriate cms claim form. This interactive guide provides instruction on how to complete the form. Ask the biller 7.16k subscribers subscribe 21k views 2 years ago this video shows you how to complete a cms 1500 claim form in. The form is used.
Completed Cms 1500 Claim Form Sample Form Resume Examples K75PBGVkl2
Insured’s address (no., street) city state zip code telephone (include area code) 11. Failure to follow these guidelines could cause a delay in processing, denial of the claim, or affect payment accuracy. And o veterans benefits (type 42). Web how to complete a cms 1500 claim form in 5 minutes! Write down the patient's full name, birth date, sex, and.

Sample Cms 1500 Form Filled Out Form Resume Examples 05KA75m8wP
Insured’s address (no., street) city state zip code telephone (include area code) 11. All items must be completed unless otherwise noted in these instructions. State the type of health insurance applicable to this claim and the insured's id number; Last updated wed, 04 jan 2023 13:36:02 +0000. Insured’s name (last name, first name, middle initial) 7.
Completed CMS 1500 form CMS 1500 claim form and UB 04 form
The center of medicaid and medicare services (cms) form 1500 is used to bill sfhp for medical services. It can be purchased in any version required by calling the u.s. This is the only format that is accepted. You'll see instructions on how to complete the field. Claims may be electronically submitted to a medicare carrier, durable medical equipment medicare.
Sample 1500 Claim Form Filled Out Form Resume Examples a15qXrADeQ
Write down the patient's full name, birth date, sex, and address. Web how to complete a cms 1500 claim form in 5 minutes! Failure to properly complete mandatory requirements will cause the claim to be denied by south dakota (sd) medicaid. All paper claims you submit must be on the appropriate cms claim form. Web the center of medicaid and.
All Items Must Be Completed Unless Otherwise Noted In These Instructions.
Number (for program in item 1) 4. Web the center of medicaid and medicare services (cms) form 1500 must be used to bill sfhp for medical services. You may also click in any field for more detailed instructions. Failure to follow these guidelines could cause a delay in processing, denial of the claim, or affect payment accuracy.
For A Paper Claim To Be Considered For Medicare Secondary Payer Benefits, A Policy Or Group Number Must Be Entered In This Item.
Last updated wed, 04 jan 2023 13:36:02 +0000. Web how to complete a cms 1500 claim form in 5 minutes! Web the 1500 health insurance claim form (1500 claim form) is in the public domain. This document is intended to be a guide for completing the 1500 claim form and not definitive instructions for this purpose.
In Addition, A Copy Of The Primary Payer’s Explanation Of Benefits (Eob) Notice Must Be
O black lung (type 41); Insured’s policy group or feca number a. Claims may be electronically submitted to a medicare carrier, durable medical equipment medicare administrative contractor (dmemac), or a/b mac from a provider's office using a computer with software that meets electronic filing requirements as established by the hipaa claim. It can be purchased in any version required by calling the u.s.
Insured’s Name (Last Name, First Name, Middle Initial) 7.
Enter the insured's full name, address, and the patient's relationship to the. Write down the patient's full name, birth date, sex, and address. The uniform claim task force introduced the form in the 1980s in an effort to standardize claims nationally, writes webpt’s melissa hughes. Failure to properly complete mandatory requirements will cause the claim to be denied by south dakota (sd) medicaid.