Cigna Provider Appeal Form 2022
Cigna Provider Appeal Form 2022 - Fields with an asterisk ( * ) are required. Web instructions please complete the below form. Web for example, over a period of two months in 2022, cigna doctors denied over 300,000 requests for payments using this method, spending an average of just 1.2. This completed form and/or an appeal letter requesting an appeal review and indicating the reason(s) why you believe the claim payment is incorrect and should be changed. Mail your appeal, payment review. Go to customer forms or, if you're a mycigna user, log in to mycigna and go to the forms center learn about appeals for medicare plans how to. Medicare advantage contracted post service appeal and claim dispute form. If you need more help,. Cigna network cigna appeals unit p.o. Be specific when completing the description of dispute and expected.
865563 05/2013 cigna is a registered service mark and the tree of. Complete the top section of this form completely and. Check the box that most closely describes your appeal or. For information about the policies and procedures for claim appeals, click the appropriate link below: Mail th iscompleted form (request for health care professional. Web if the id card indicates: Fields with an asterisk ( * ) are required. Contracted post service appeal and claim dispute form [pdf] contracted post service appeal and claim dispute form [pdf] (az only) non. If you have multiple reconsideration requests for the same health care professional and payment issue, please indicate this in the notes below and include a list. Web to allow us the opportunity to provide a full and thorough review, health care professionals should submit complete information with their appeal.
Web if the id card indicates: Web cigna medicare advantage plans. Health care professionals provider manual. Check the box that most closely describes your appeal or. For information about the policies and procedures for claim appeals, click the appropriate link below: Cigna network cigna appeals unit p.o. Be specific when completing the description of dispute and expected. Complete the top section of this form completely and. Web updated march 2021 registered users of the cigna for health care professionals website (cignaforhcp.com) have the ability to submit and check the status of appeals and claim. Web include a provider appealing on his/her behalf) may appeal the adverse decision related to your coverage.

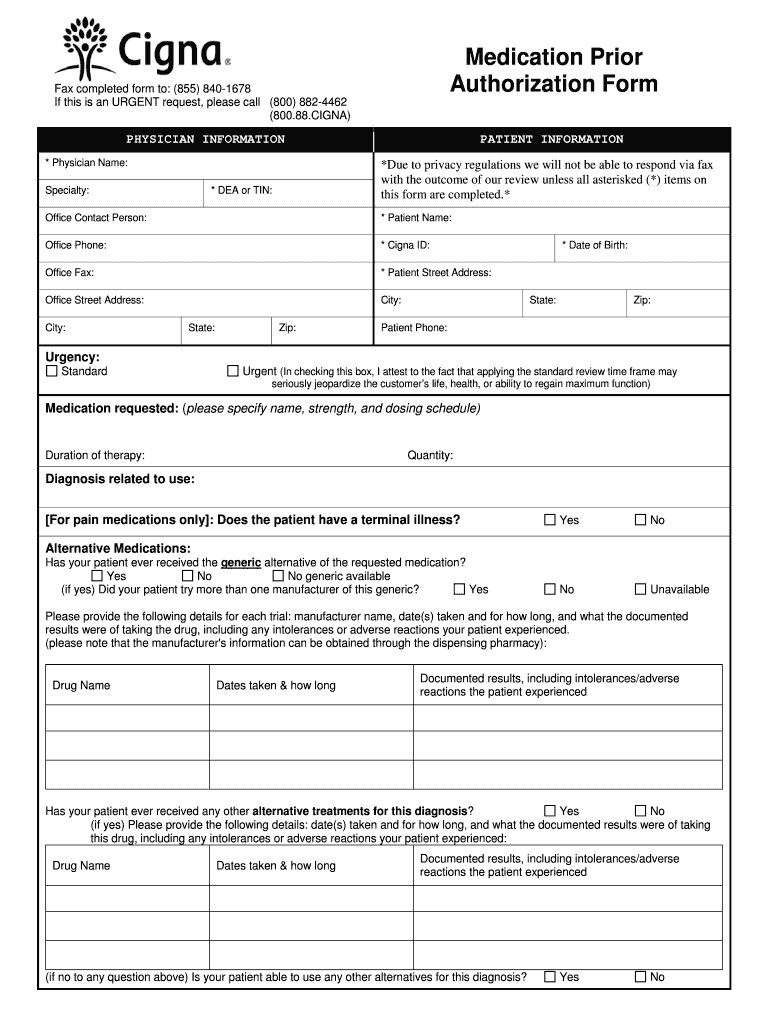
Cigna Medical Request Form 20202021 Fill and Sign Printable Template
Cigna healthcare appeal policy and procedures. If you need more help,. Web instructions please complete the below form. Mail your appeal, payment review. Go to customer forms or, if you're a mycigna user, log in to mycigna and go to the forms center learn about appeals for medicare plans how to.
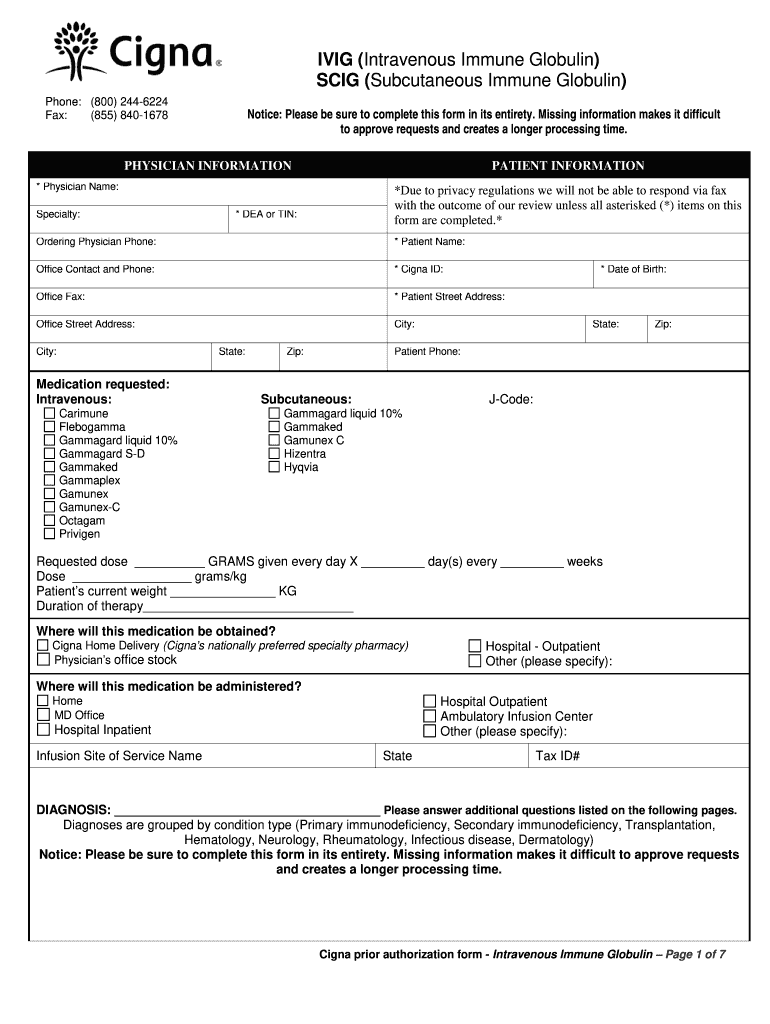
Cigna ivig prior authorization form Fill out & sign online DocHub
Cigna network cigna appeals unit p.o. Your appeal should be submitted within. Go to customer forms or, if you're a mycigna user, log in to mycigna and go to the forms center learn about appeals for medicare plans how to. Be specific when completing the description of dispute and expected. If you need more help,.
Health Plan of San Mateo Prior Authorization Form Fill Out and Sign
Web appeals and reconsideration request form complete the top section of this form completely and legibly. Web complete and mail this form and/or appeal letter along with all supporting documentation to the address identified in step 3 on this form. Web health care provider (practitioner/facility name): Contracted post service appeal and claim dispute form [pdf] contracted post service appeal and.

Cigna Appeal Request Fill and Sign Printable Template Online US
Web for example, over a period of two months in 2022, cigna doctors denied over 300,000 requests for payments using this method, spending an average of just 1.2. Go to customer forms or, if you're a mycigna user, log in to mycigna and go to the forms center learn about appeals for medicare plans how to. Complete the top section.

International Student Health Insurance Plan (ISHIP) Relation
Web health care provider (practitioner/facility name): Fields with an asterisk ( * ) are required. Web to file an appeal or grievance: Web cigna medicare advantage plans. If you have multiple reconsideration requests for the same health care professional and payment issue, please indicate this in the notes below and include a list.

Cigna 360 exam
Verify coverage call cigna at the number listed on the back of the covered individual's id card or log in to the cigna for health care professionals website at. Complete the top section of this form completely and. Contracted post service appeal and claim dispute form [pdf] contracted post service appeal and claim dispute form [pdf] (az only) non. Go.
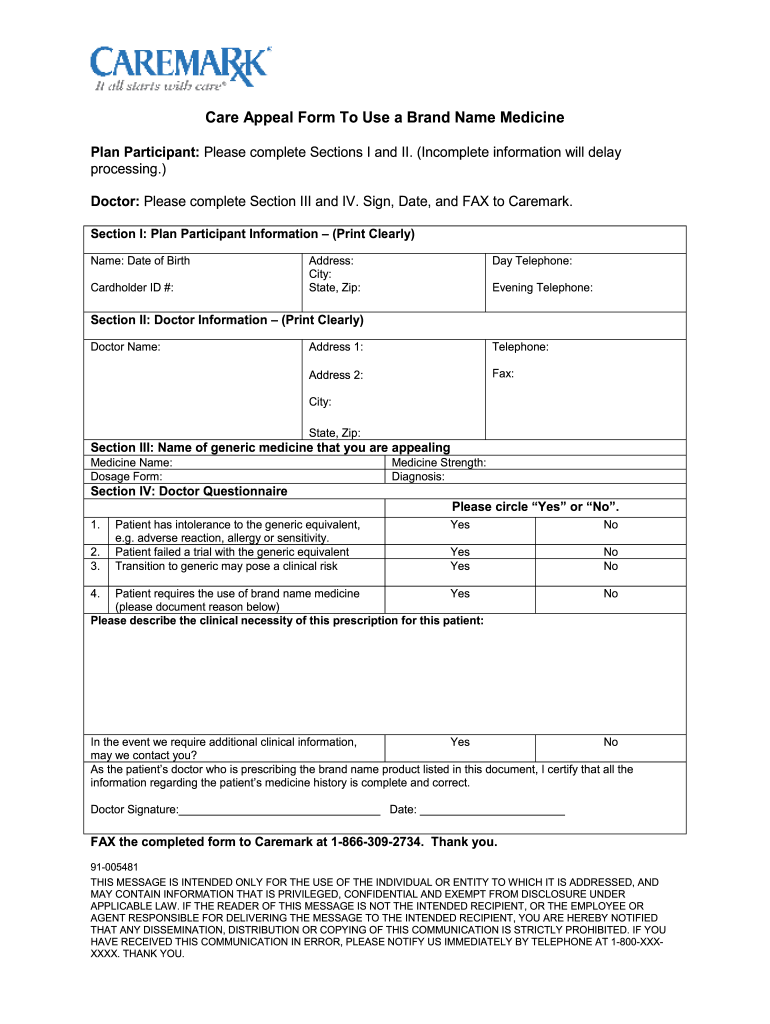
Cvs Caremark Appeal Form Fill Out and Sign Printable PDF Template
Web last updated 10/01/2022. Complete the top section of this form completely and. For information about the policies and procedures for claim appeals, click the appropriate link below: Be specific when completing the description of dispute and expected. Web find appeal policies, claim editing procedures and laboratory and reimbursement information critical to working with cigna.
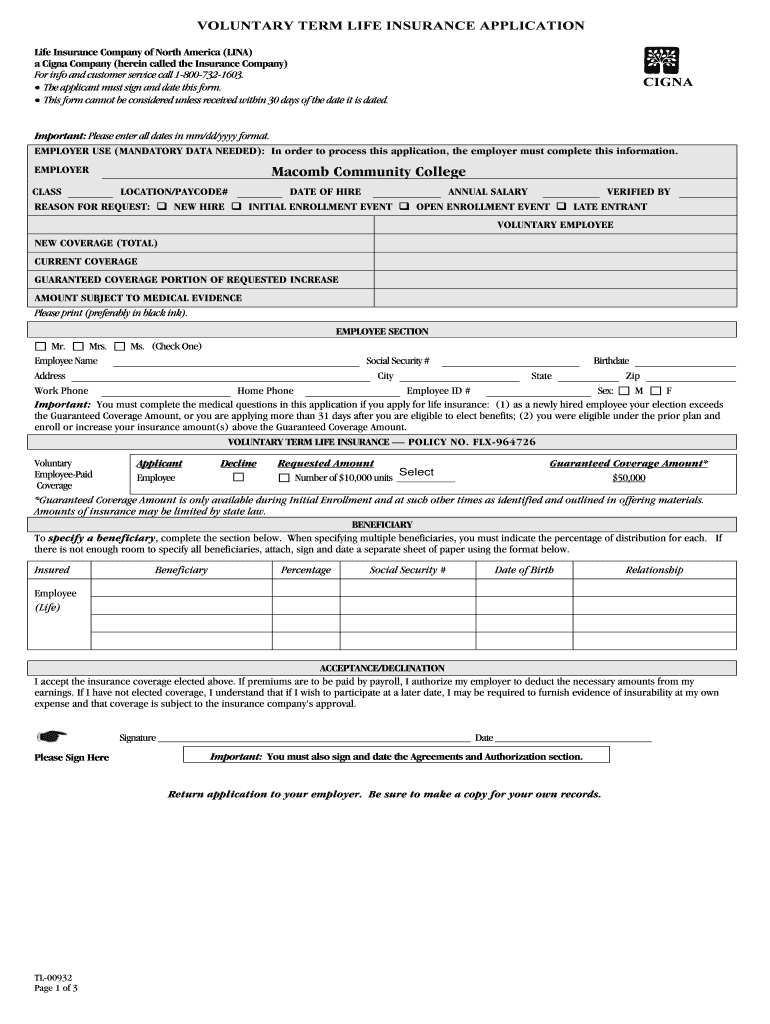
Cigna TL00932 Fill and Sign Printable Template Online US Legal Forms
Medicare advantage contracted post service appeal and claim dispute form. Check the box that most closely describes your appeal or. Web instructions please complete the below form. If you need more help,. This completed form and/or an appeal letter requesting an appeal review and indicating the reason(s) why you believe the claim payment is incorrect and should be changed.
Molina Medication Prior Form Fill Out and Sign Printable PDF Template
Web for example, over a period of two months in 2022, cigna doctors denied over 300,000 requests for payments using this method, spending an average of just 1.2. 865563 05/2013 cigna is a registered service mark and the tree of. Ad cigna appeal request & more fillable forms, register and subscribe now! Cigna network cigna appeals unit p.o. Web to.

Medicare Redetermination Form 2020 2020 Fill and Sign Printable
Go to customer forms or, if you're a mycigna user, log in to mycigna and go to the forms center learn about appeals for medicare plans how to. If you have multiple reconsideration requests for the same health care professional and payment issue, please indicate this in the notes below and include a list. Mail th iscompleted form (request for.
Web Find Appeal Policies, Claim Editing Procedures And Laboratory And Reimbursement Information Critical To Working With Cigna.
Web if the id card indicates: If you need more help,. Contracted post service appeal and claim dispute form [pdf] contracted post service appeal and claim dispute form [pdf] (az only) non. Medicare advantage contracted post service appeal and claim dispute form.
Web Updated March 2021 Registered Users Of The Cigna For Health Care Professionals Website (Cignaforhcp.com) Have The Ability To Submit And Check The Status Of Appeals And Claim.
Web complete and mail this form and/or appeal letter along with all supporting documentation to the address identified in step 3 on this form. For information about the policies and procedures for claim appeals, click the appropriate link below: Check the box that most. Go to customer forms or, if you're a mycigna user, log in to mycigna and go to the forms center learn about appeals for medicare plans how to.
Your Appeal Should Be Submitted Within.
This completed form and/or an appeal letter requesting an appeal review and indicating the reason(s) why you believe the claim payment is incorrect and should be changed. You’ll send this form to the same place where you are sending your grievance, coverage determination, or appeal. Cigna healthcare appeal policy and procedures. Web instructions please complete the below form.
Fields With An Asterisk ( * ) Are Required.
Web to allow us the opportunity to provide a full and thorough review, health care professionals should submit complete information with their appeal. Complete the top section of this form completely and. Check the box that most closely describes your appeal or. Web cigna medicare advantage non contracted provider appeals and disputes form complete the top section of this form completely and legibly.