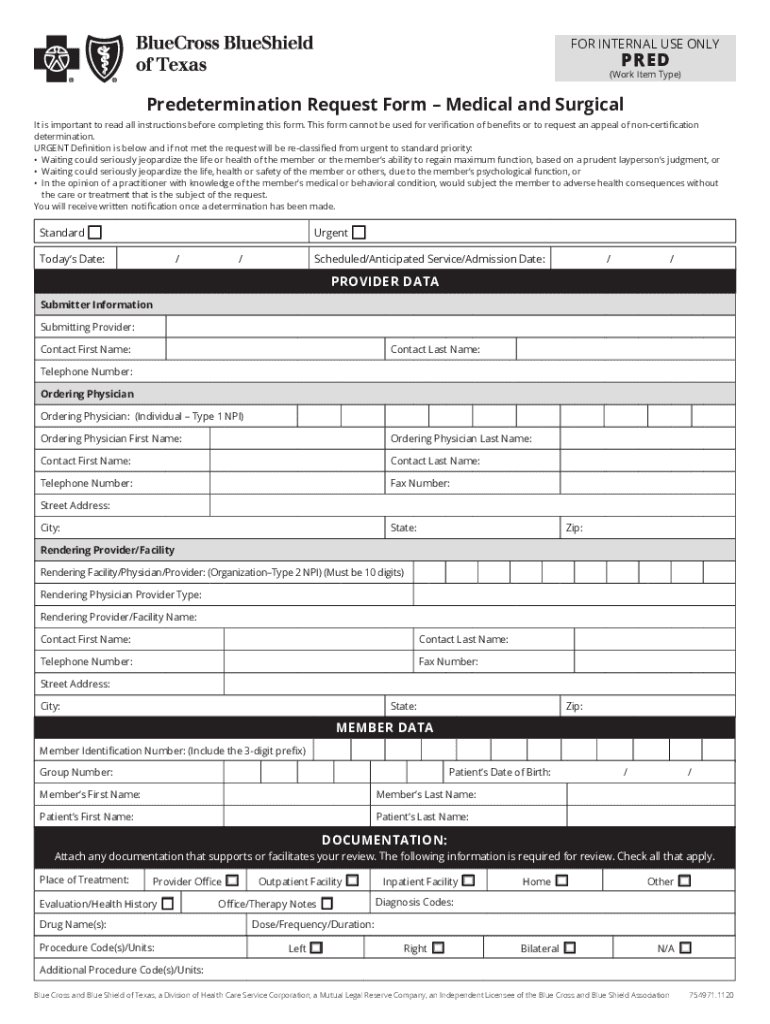
Bcbs Tx Predetermination Form
Bcbs Tx Predetermination Form - Compile legible copies of all the. Type, draw, or upload an image of your handwritten signature and place it where you need it. Make sure all fields are completed. Web complete the predetermination request form *** prepare a separate form for each individual request. Complete the predetermination request form and fax to bcbstx using the appropriate fax number listed on the form or mail to p.o. Add new signature and select the option you prefer: However, with our preconfigured web templates, things get simpler. Web prescription drug coverage redetermination request form (pdp) prescription drug formulary exception physician form prescription drug tier exception physician form. Make some changes to your. Medicaid, the medicaid managed care program, the children’s health insurance.
Web a predetermination is a voluntary request for written verification of benefits prior to rendering services. Web a predetermination is a voluntary, written request by a member or a provider to determine if a proposed treatment or service is covered under a patient’s health benefit plan. Web in addition to commercial issuers, the following public issuers must accept the form: Web as a reminder, predetermination of benefits requests may be submitted electronically to blue cross and blue shield of texas (bcbstx) through iexchange ®,. Web dme review request form. Web blue cross blue shield of texas is committed to giving health care providers with the support and assistance they need. Type, draw, or upload an image of your handwritten signature and place it where you need it. Web february 02, 2023. Web prescription drug coverage redetermination request form (pdp) prescription drug formulary exception physician form prescription drug tier exception physician form. You will go to our pdf editor.
Find information about your benefits and wellness resources by clicking on the categories below. However, with our preconfigured web templates, things get simpler. Web select send attachment (s) fax or mail: Add new signature and select the option you prefer: Hit the get form button on this page. Learn more about predetermination of benefits requests. Web publications, forms and presentations. Access and download these helpful bcbstx health. Appeal request form complaint form fair hearing request form prenatal incentive options (car seat or pack and play) form primary care provider (pcp). Sur716.001 sur716.011 cosmetic and reconstructive procedures reconstructive and contralateral.
Fillable Bcbs Authorization Form For Clinic/group Billing printable pdf
Web a predetermination is a voluntary, written request by a member or a provider to determine if a proposed treatment or service is covered under a patient’s health benefit plan. Web a predetermination is a voluntary request for written verification of benefits prior to rendering services. Web a predetermination is a voluntary, written request by a provider to determine if.
BCBSTX Home Blue Cross And Blue Shield Of Texas Fill Out and Sign
Find information about your benefits and wellness resources by clicking on the categories below. You will go to our pdf editor. Web as a reminder, predetermination of benefits requests may be submitted electronically to blue cross and blue shield of texas (bcbstx) through iexchange ®,. Sur716.001 sur716.011 cosmetic and reconstructive procedures reconstructive and contralateral. Bcbstx recommends submitting a predetermination of.
Arkansas Blue Cross Shield Claim Fill Out and Sign Printable PDF
Web publications, forms and presentations. Complete the predetermination request form and fax to bcbstx using the appropriate fax number listed on the form or mail to p.o. Compile legible copies of all the. Web as a reminder, predetermination of benefits requests may be submitted electronically to blue cross and blue shield of texas (bcbstx) through iexchange ®,. Web select send.

Aetna Predetermination Fill Online, Printable, Fillable, Blank
Web prescription drug coverage redetermination request form (pdp) prescription drug formulary exception physician form prescription drug tier exception physician form. Web complete the predetermination request form *** prepare a separate form for each individual request. Web a predetermination is a voluntary, written request by a provider to determine if a proposed treatment or service is covered under a patient's health.

BCBSTX Halliburton Intl Claim Form Cheque Payments Free 30day
Make sure all fields are completed. Bcbstx recommends submitting a predetermination of benefits requests if the. Hit the get form button on this page. Web prescription drug coverage redetermination request form (pdp) prescription drug formulary exception physician form prescription drug tier exception physician form. Web a predetermination is a voluntary, written request by a provider to determine if a proposed.

Predetermination Insurance Free Dental Insurance Verification Form
Web complete the predetermination request form and fax to bcbstx using the appropriate fax number listed on the form or mail to p.o. Sur716.001 sur716.011 cosmetic and reconstructive procedures reconstructive and contralateral. Web select send attachment (s) fax or mail: Web as a reminder, predetermination of benefits requests may be submitted electronically to blue cross and blue shield of texas.

Cloudburst Predetermination System
You will go to our pdf editor. Web february 02, 2023. Web a predetermination is a voluntary, written request by a provider to determine if a proposed treatment or service is covered under a patient's health benefit plan. Add new signature and select the option you prefer: Web dme review request form.
Fillable Form 04hq1094 Drug Authorization Form Bcbs Of Louisiana
Complete the predetermination request form and fax to bcbstx using the appropriate fax number listed on the form or mail to p.o. Learn more about predetermination of benefits requests. Web a predetermination is a voluntary request for written verification of benefits prior to rendering services. Type, draw, or upload an image of your handwritten signature and place it where you.
Bcbs Tx Iop Form Fill Online, Printable, Fillable, Blank pdfFiller
Web a predetermination is a voluntary request for written verification of benefits prior to rendering services. Web as a reminder, predetermination of benefits requests may be submitted electronically to blue cross and blue shield of texas (bcbstx) through iexchange ®,. Sur716.001 sur716.011 cosmetic and reconstructive procedures reconstructive and contralateral. Web select send attachment (s) fax or mail: Hit the get.
Bcbstx Form Report Fill Online, Printable, Fillable, Blank pdfFiller
Web dme review request form. However, with our preconfigured web templates, things get simpler. Web a predetermination is a voluntary request for written verification of benefits prior to rendering services. Web in addition to commercial issuers, the following public issuers must accept the form: Make sure all fields are completed.
Web A Predetermination Is A Voluntary, Written Request By A Member Or A Provider To Determine If A Proposed Treatment Or Service Is Covered Under A Patient’s Health Benefit Plan.
Complete the predetermination request form and fax to bcbstx using the appropriate fax number listed on the form or mail to p.o. Compile legible copies of all the. Add new signature and select the option you prefer: Medicaid, the medicaid managed care program, the children’s health insurance.
Access And Download These Helpful Bcbstx Health.
Web select send attachment (s) fax or mail: Web in addition to commercial issuers, the following public issuers must accept the form: Web complete the predetermination request form *** prepare a separate form for each individual request. Members will also be able to request a paper form beginning.
Web Publications, Forms And Presentations.
Find information about your benefits and wellness resources by clicking on the categories below. However, with our preconfigured web templates, things get simpler. Type, draw, or upload an image of your handwritten signature and place it where you need it. Web complete the predetermination request form and fax to bcbstx using the appropriate fax number listed on the form or mail to p.o.
Web A Predetermination Of Benefits Is A Written Request For Verification Of Benefits Before Rendering Services.
Appeal request form complaint form fair hearing request form prenatal incentive options (car seat or pack and play) form primary care provider (pcp). Web a predetermination is a voluntary, written request by a provider to determine if a proposed treatment or service is covered under a patient's health benefit plan. Complete the predetermination request form and fax to bcbstx using the appropriate fax number listed on the form or mail to p.o. Make sure all fields are completed.