Bcbs Clinical Appeal Form
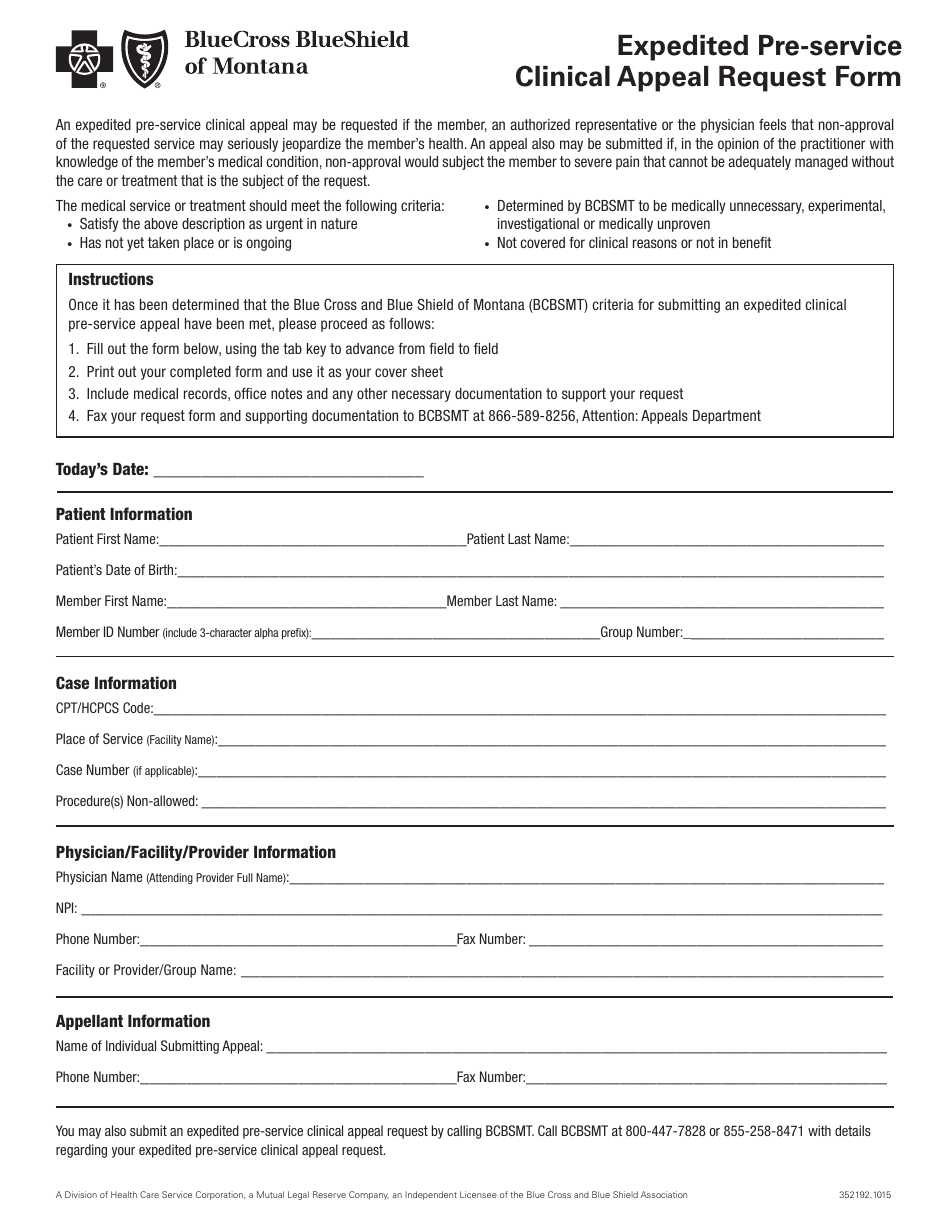
Bcbs Clinical Appeal Form - Please review the instructions for each category below to ensure proper routing of your appeal. Web the provider clinical appeal form should be used when clinical decision making is necessary: Check the appropriate box for the utilization management appeal reason, either “authorization” or “precertification”; Check the “utilization management” box under appeal type; When not to submit an appeal. Appeals are divided into two categories: Web florida blue members can access a variety of forms including: Web electronic clinical claim appeal request via availity ® the dispute tool allows providers to electronically submit appeal requests for specific clinical claim denials through the availity portal. When to submit an appeal. Review is conducted by a physician.
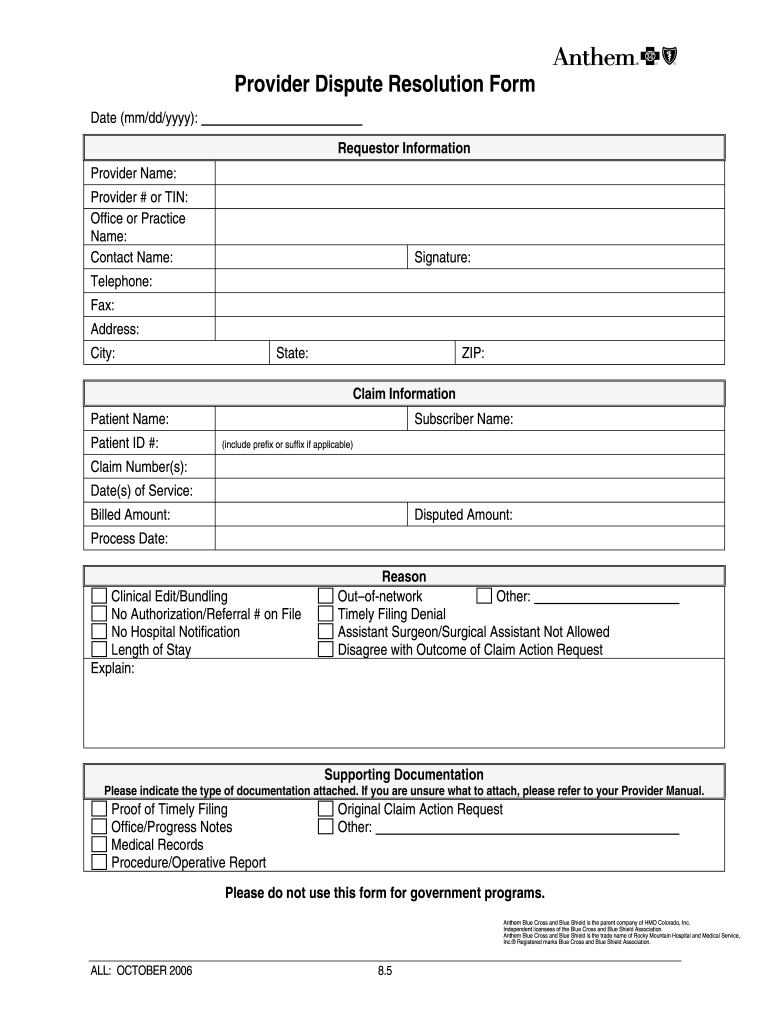
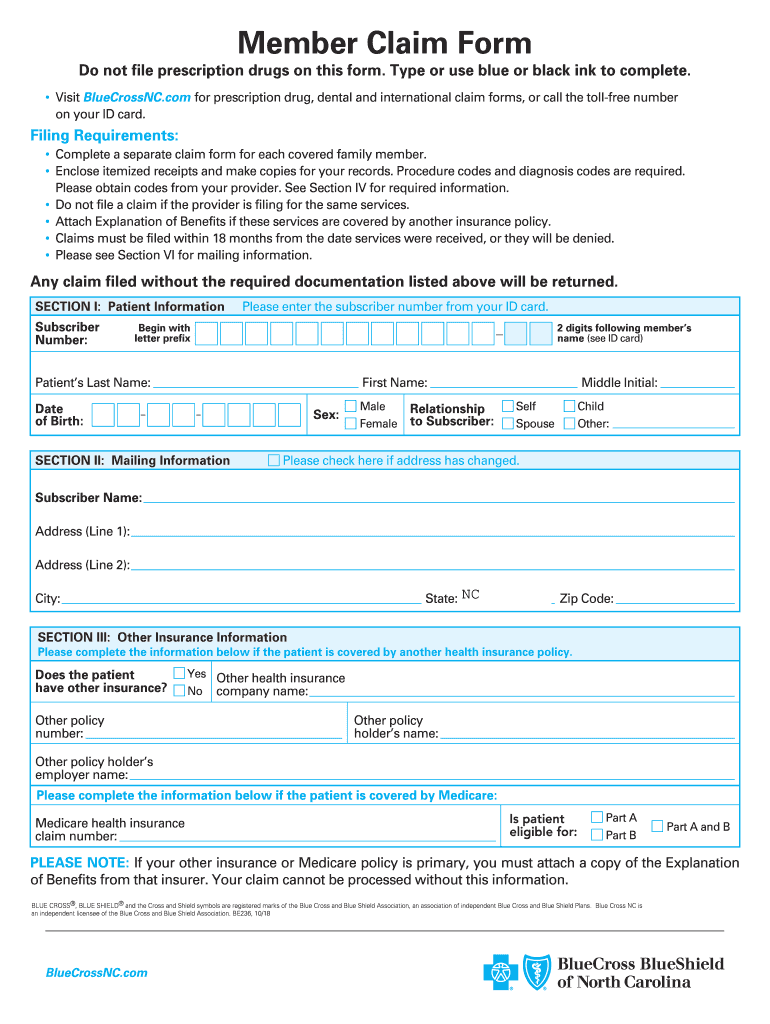
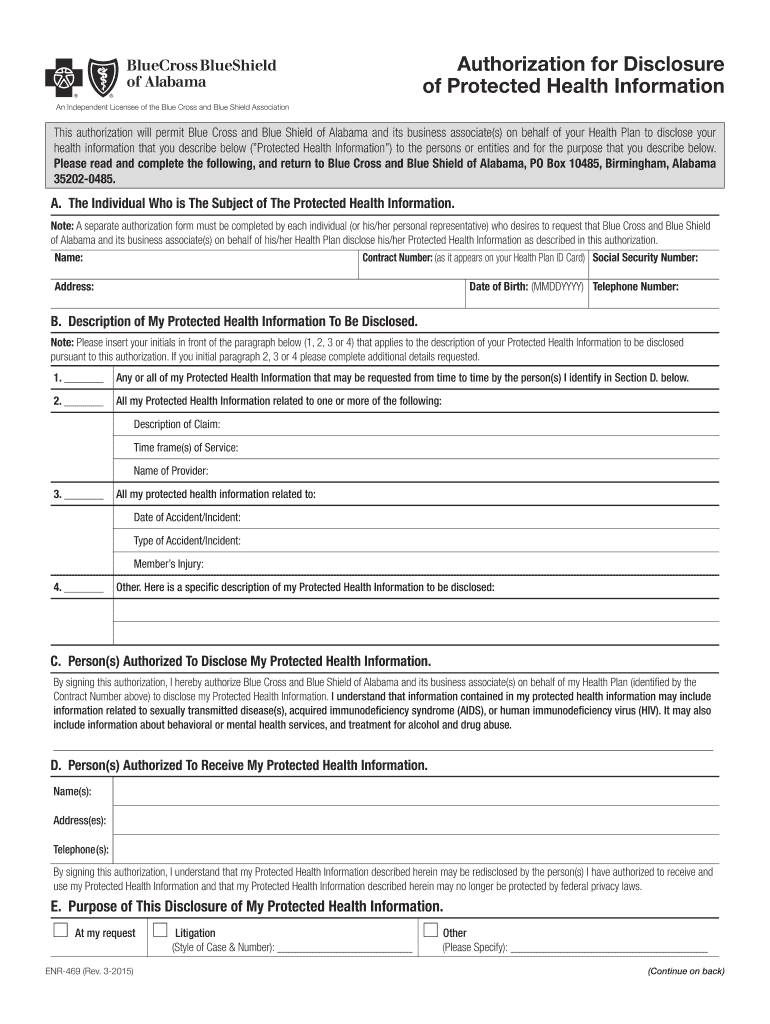
Medical claims, vision claims and reimbursement forms, prescription drug forms, coverage and premium payment and personal information. Date _____ provider reconsideration administrative appeal (must include reconsideration #) _____ reason for provider reconsideration request / administrative appeal (check one) claim allowance Check the appropriate box for the utilization management appeal reason, either “authorization” or “precertification”; Web the provider clinical appeal form should be used when clinical decision making is necessary: Utilization management adverse determination coding and payment rule please review the instructions for each category below to ensure proper routing of your appeal. Review is conducted by a physician. Web a clinical appeal is a request to change an adverse determination for care or services that were denied on the basis of lack of medical necessity, or when services are determined to be experimental, investigational or cosmetic. Please review the instructions for each category below to ensure proper routing of your appeal. Web florida blue members can access a variety of forms including: Appeals are divided into two categories:
Please send only one claim per form. Check the “utilization management” box under appeal type; Bcn advantage appeals and grievance unit p.o. Web appeals must be submitted within one year from the date on the remittance advice. Utilization management adverse determination coding and payment rule please review the instructions for each category below to ensure proper routing of your appeal. Web provider appeal form instructions physicians and providers may appeal how a claim processed, paid or denied. When not to submit an appeal. Web a clinical appeal is a request to change an adverse determination for care or services that were denied on the basis of lack of medical necessity, or when services are determined to be experimental, investigational or cosmetic. Web the provider clinical appeal form should be used when clinical decision making is necessary: Web florida blue members can access a variety of forms including:

TN BCBS 17PED153727 20172021 Fill and Sign Printable Template Online
Web provider appeal form instructions physicians and providers may appeal how a claim processed, paid or denied. Please review the instructions for each category below to ensure proper routing of your appeal. And enter the authorization or precertification. Check the appropriate box for the utilization management appeal reason, either “authorization” or “precertification”; Review is conducted by a physician.
Anthem provider dispute form Fill out & sign online DocHub
Date _____ provider reconsideration administrative appeal (must include reconsideration #) _____ reason for provider reconsideration request / administrative appeal (check one) claim allowance Medical claims, vision claims and reimbursement forms, prescription drug forms, coverage and premium payment and personal information. Web a clinical appeal is a request to change an adverse determination for care or services that were denied on.
Nc Bcbs Form Fill Out and Sign Printable PDF Template signNow
Bcn advantage appeals and grievance unit p.o. Date _____ provider reconsideration administrative appeal (must include reconsideration #) _____ reason for provider reconsideration request / administrative appeal (check one) claim allowance When to submit an appeal. Web appeals must be submitted within one year from the date on the remittance advice. When applicable, the dispute option is.

Bcbs Federal Provider Appeal form Best Of Fep Prior Authorization form â
Web florida blue members can access a variety of forms including: Bcn advantage appeals and grievance unit p.o. When to submit an appeal. Web a clinical appeal is a request to change an adverse determination for care or services that were denied on the basis of lack of medical necessity, or when services are determined to be experimental, investigational or.
Form 352192.1015 Download Fillable PDF or Fill Online Expedited Pre
Web florida blue members can access a variety of forms including: When not to submit an appeal. Date _____ provider reconsideration administrative appeal (must include reconsideration #) _____ reason for provider reconsideration request / administrative appeal (check one) claim allowance Web a clinical appeal is a request to change an adverse determination for care or services that were denied on.
Bcbs Of Alabama Prior Authorization Fill Out and Sign Printable PDF
Web the provider clinical appeal form should be used when clinical decision making is necessary: Please send only one claim per form. When to submit an appeal. Medical claims, vision claims and reimbursement forms, prescription drug forms, coverage and premium payment and personal information. Review is conducted by a physician.

Bcbs Federal Provider Appeal form Elegant Service Dog Letter Template
Web a clinical appeal is a request to change an adverse determination for care or services that were denied on the basis of lack of medical necessity, or when services are determined to be experimental, investigational or cosmetic. When applicable, the dispute option is. Web electronic clinical claim appeal request via availity ® the dispute tool allows providers to electronically.
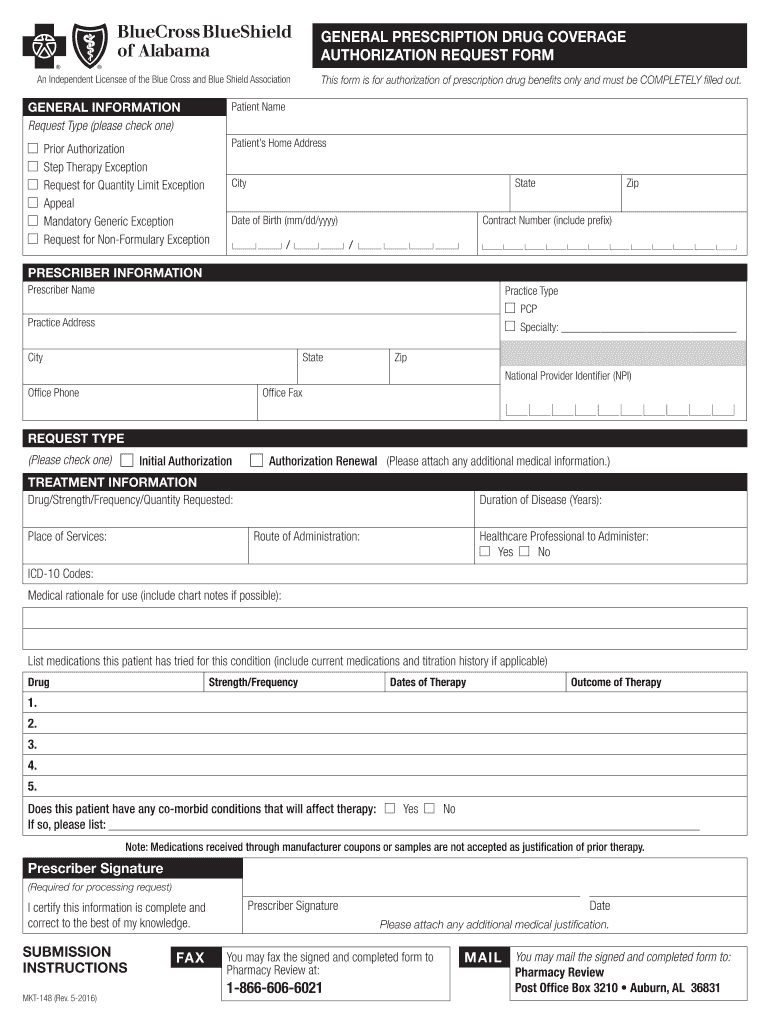
Bcbs Alabama Prior Authorization Form Fill Out and Sign Printable PDF
When to submit an appeal. Date _____ provider reconsideration administrative appeal (must include reconsideration #) _____ reason for provider reconsideration request / administrative appeal (check one) claim allowance Please review the instructions for each category below to ensure proper routing of your appeal. Utilization management adverse determination coding and payment rule please review the instructions for each category below to.
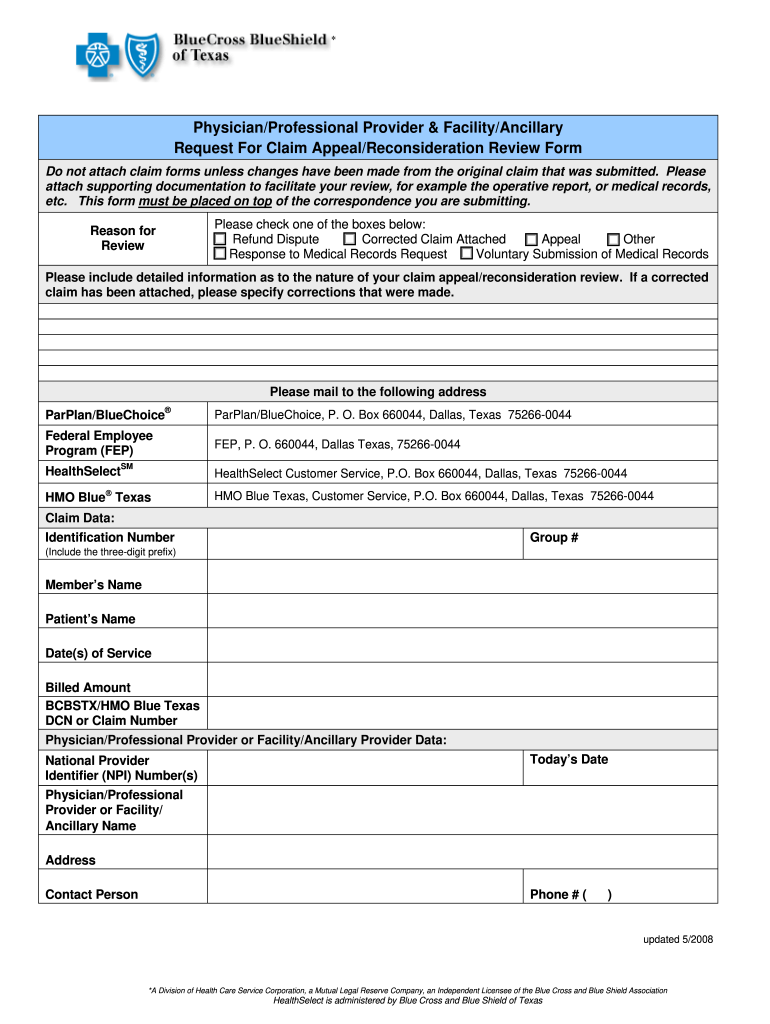
Texas Bcbs Provider Appeal Fill Out and Sign Printable PDF Template
Utilization management adverse determination coding and payment rule please review the instructions for each category below to ensure proper routing of your appeal. And enter the authorization or precertification. Check the appropriate box for the utilization management appeal reason, either “authorization” or “precertification”; When applicable, the dispute option is. When to submit an appeal.
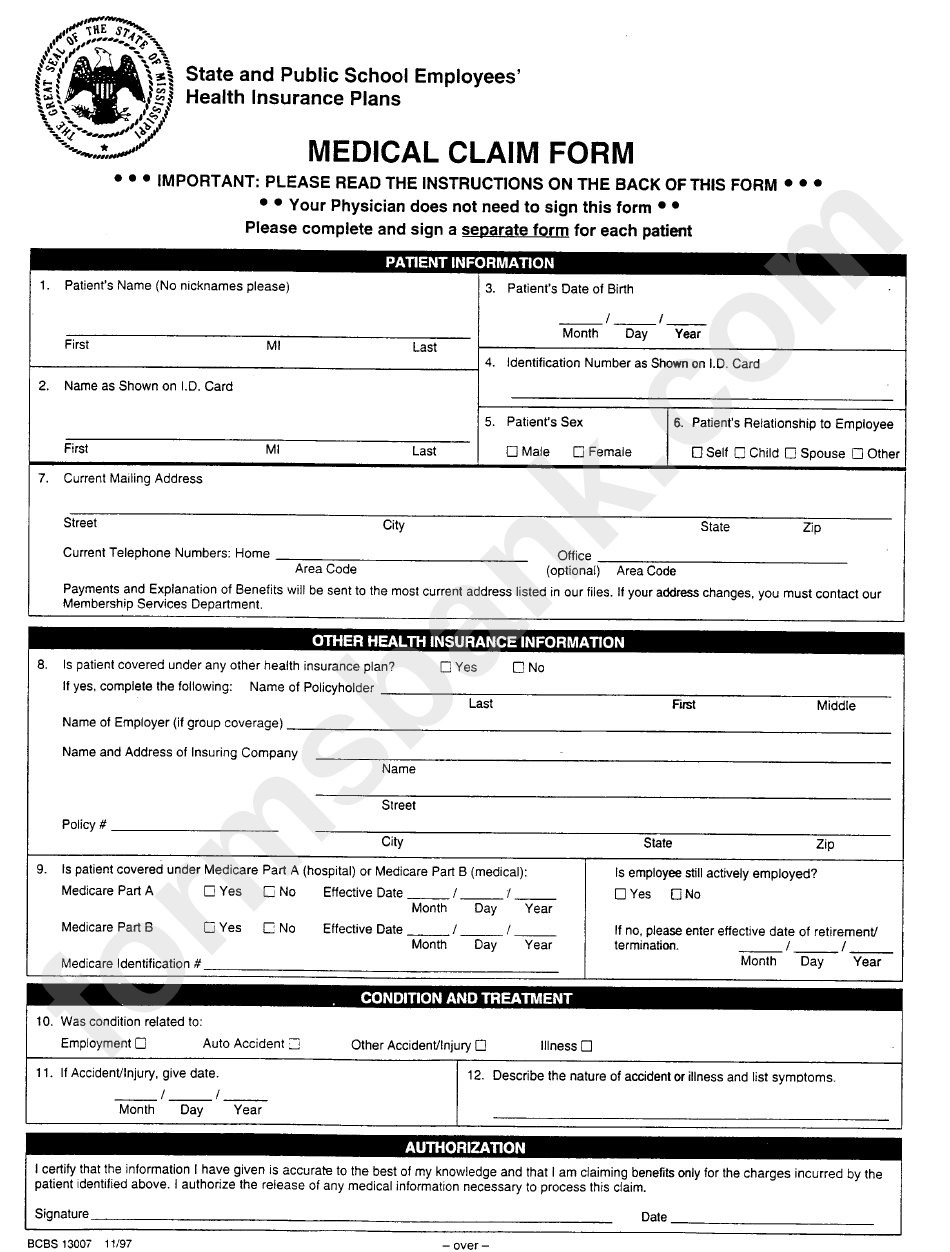
Form Bcbs 13007 State And Public School Employees Medical Claim Form
Web electronic clinical claim appeal request via availity ® the dispute tool allows providers to electronically submit appeal requests for specific clinical claim denials through the availity portal. Date _____ provider reconsideration administrative appeal (must include reconsideration #) _____ reason for provider reconsideration request / administrative appeal (check one) claim allowance Web a clinical appeal is a request to change.
Bcn Advantage Appeals And Grievance Unit P.o.
Check the “utilization management” box under appeal type; Check the appropriate box for the utilization management appeal reason, either “authorization” or “precertification”; Web appeals must be submitted within one year from the date on the remittance advice. Medical claims, vision claims and reimbursement forms, prescription drug forms, coverage and premium payment and personal information.
Please Send Only One Claim Per Form.
When applicable, the dispute option is. Utilization management adverse determination coding and payment rule please review the instructions for each category below to ensure proper routing of your appeal. Date _____ provider reconsideration administrative appeal (must include reconsideration #) _____ reason for provider reconsideration request / administrative appeal (check one) claim allowance When to submit an appeal.
When Not To Submit An Appeal.
Please review the instructions for each category below to ensure proper routing of your appeal. Web provider appeal form instructions physicians and providers may appeal how a claim processed, paid or denied. Web electronic clinical claim appeal request via availity ® the dispute tool allows providers to electronically submit appeal requests for specific clinical claim denials through the availity portal. Review is conducted by a physician.
Web The Provider Clinical Appeal Form Should Be Used When Clinical Decision Making Is Necessary:
Web florida blue members can access a variety of forms including: Web a clinical appeal is a request to change an adverse determination for care or services that were denied on the basis of lack of medical necessity, or when services are determined to be experimental, investigational or cosmetic. And enter the authorization or precertification. Appeals are divided into two categories: