Ada Claim Form 2019 Pdf
Ada Claim Form 2019 Pdf - 2019 ada dental claim form as the replacement for the 2012 and 2018 ada dental claim form. This is the most recent version of the form. The ada dental claim form and the cdt manual are copyrighted documents. Add the printable 2019 ada claim form for redacting. Web the american dental association (ada) has approved the new. Enter your official contact and identification details. Employer name patient information 18. Sign up and log in to your account. Dental claim form completion instructions can be found on the ada’s web site. Web ada 2019 claim form for licensees the ada dental claim form was last structurally revised in 2012 to incorporate key data content changes that enables diagnosis code reporting that was also incorporated into the now current version of the hipaa standard (837d v5010) electronic dental claim.
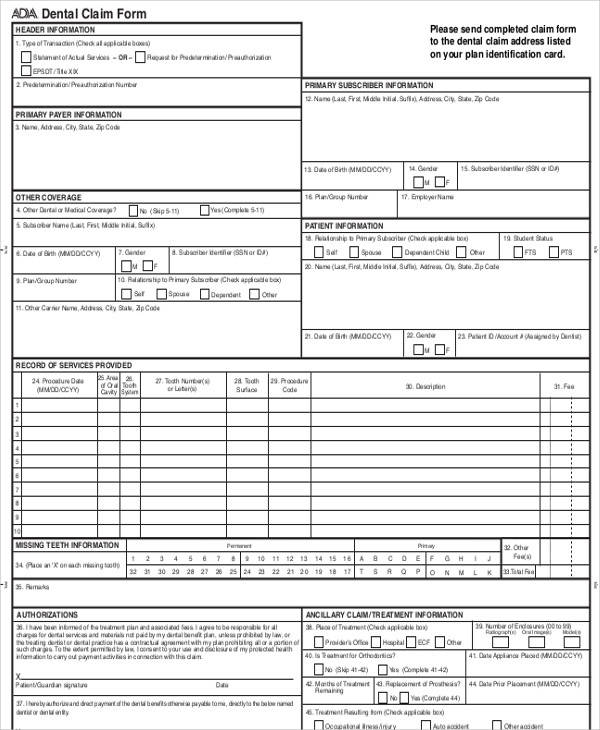
Web ada 2019 claim form for licensees the ada dental claim form was last structurally revised in 2012 to incorporate key data content changes that enables diagnosis code reporting that was also incorporated into the now current version of the hipaa standard (837d v5010) electronic dental claim. Numberof enclosures (00 to 99) charges for dental services and materials not paid by my dental benefit plan, unless prohibited by law, or o Web check out the ada online store for dental claim form (2019 version) downloadable pdf. Web dental claim form statement of actual services request for predetermination/preauthorization epsdt / title xix 2. Dental claim form completion instructions can be found on the ada’s web site. Vha office of community care. Ada dental claim form instructions. Web this pdf editor makes it easy to fill out the ada dental claim form 2019 document. The ada dental claim form and the cdt manual are copyrighted documents. Web ada dental claim form ada american dental association0 header information 1.
Web 2019 ada dental claim form. Web this pdf editor makes it easy to fill out the ada dental claim form 2019 document. The following information highlights certain va specific form completion instructions. The ada dental claim form and the cdt manual are copyrighted documents. Sign up and log in to your account. Web the ada dental claim form provides a common format for reporting dental services to a patient's dental benefit plan. Web object moved this document may be found here Employer name patient information 18. Dental claim form completion instructions can be found on the ada’s web site. 2019 ada dental claim form as the replacement for the 2012 and 2018 ada dental claim form.
Dental Paper Claim Forms Fiachra Forms Charting Solutions
Web this pdf editor makes it easy to fill out the ada dental claim form 2019 document. Dental claim form completion instructions can be found on the ada’s web site. Web check out the ada online store for dental claim form (2019 version) downloadable pdf. This is the most recent version of the form. Numberof enclosures (00 to 99) charges.

Where does box 56a on the ADA claim form come from? Dentrix Ascend
Web authorizations ancillary claim/treatment information 36. Date of birth (mm/dd/ccyy) 14. Numberof enclosures (00 to 99) charges for dental services and materials not paid by my dental benefit plan, unless prohibited by law, or o You will be able to obtain the form effortlessly through using these simple actions. Dental claim form completion instructions can be found on the ada’s.

J430 Dental Claim Form Healthcare Claims OCR for CMS1500, UB04 & J430
Predetermination/preauthorization number dental benefit plan information 3. Gender15.policyholder/subscriber id (assigned by plan) nmnfnu 16. The ada dental claim form and the cdt manual are copyrighted documents. To get started on the form, utilize the fill camp; Web 2019 ada dental claim form.
Medicare Claim Form Printable Master of Documents
Comprehensive ada dental claim form completion instructions are printed in the cdt manual. The illustrations are then followed by comprehensive form completion instructions. Numberof enclosures (00 to 99) charges for dental services and materials not paid by my dental benefit plan, unless prohibited by law, or o The ada dental claim form was revised in 2019 with editorial changes to.
ADA Store Dental Claim Form (2019 Version) Downloadable PDF
Enter your official contact and identification details. You will be able to obtain the form effortlessly through using these simple actions. 63 services and items requiring 1150 administrative waiver. Vha office of community care. Sign online button or tick the preview image of the blank.

Dental Software DentiMax C Clickable 1999 ADA Claim Form
This is the most recent version of the form. Date of birth (mm/dd/ccyy) 14. Company/plan name, address, city, state, zip code fold fold policyholder/subscriber information (assigned by. Numberof enclosures (00 to 99) charges for dental services and materials not paid by my dental benefit plan, unless prohibited by law, or o To get started on the form, utilize the fill.

8 crucial ADA claim form boxes eAssist Dental Billing
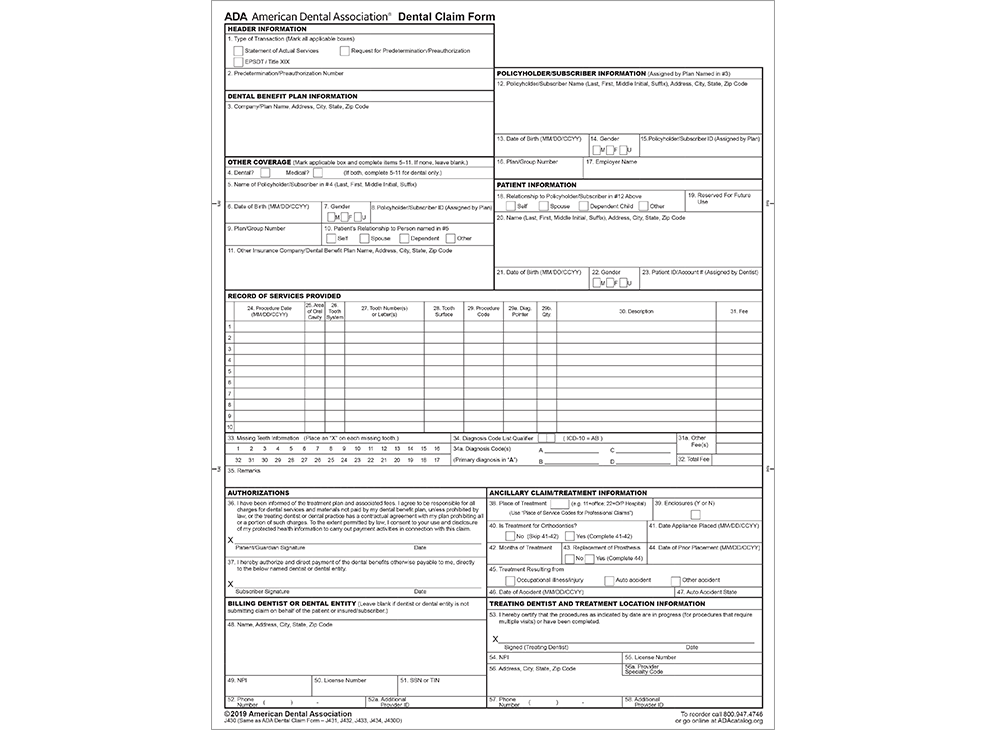
Web this pdf editor makes it easy to fill out the ada dental claim form 2019 document. Web summary of form version 2019 editorial and completion instruction changes the current version of the paper form (2019 © american dental association), front and reverse sides, is illustrated on the next two pages. Date of birth (mm/dd/ccyy) 14. Company/plan name, address, city,.
Office Support
Comprehensive ada dental claim form completion instructions. The ada dental claim form was revised in 2019 with editorial changes to form captions and check box options for gender (m, f and u) to be consistent with the hipaa standard electronic dental claim (837d). Enter your official contact and identification details. Web summary of form version 2019 editorial and completion instruction.

2019 New ADA Dental Claim Form WADA2019CS StockChecks
Predetermination/preauthorization number request for predetermination/preauthorization policyholder/subscriber information. Web summary of form version 2019 editorial and completion instruction changes the current version of the paper form (2019 © american dental association), front and reverse sides, is illustrated on the next two pages. Company/plan name, address, city, state, zip code fold fold policyholder/subscriber information (assigned by. Ada dental claim form instructions. I.
Printable Ada Dental Claim Form 2019 Printable Word Searches
To get started on the form, utilize the fill camp; Choose the button get form here. Sign in to the editor with your credentials or click on create free account to examine the tool’s functionality. The ada dental claim form was revised in 2019 with editorial changes to form captions and check box options for gender (m, f and u).
Employer Name Patient Information 18.
Web check out the ada online store for dental claim form (2019 version) downloadable pdf. Ada dental claim form instructions. Policyholder/subscriber name (last, first, middle initial, suffix), address, city, state, zip code 13. Enter your official contact and identification details.
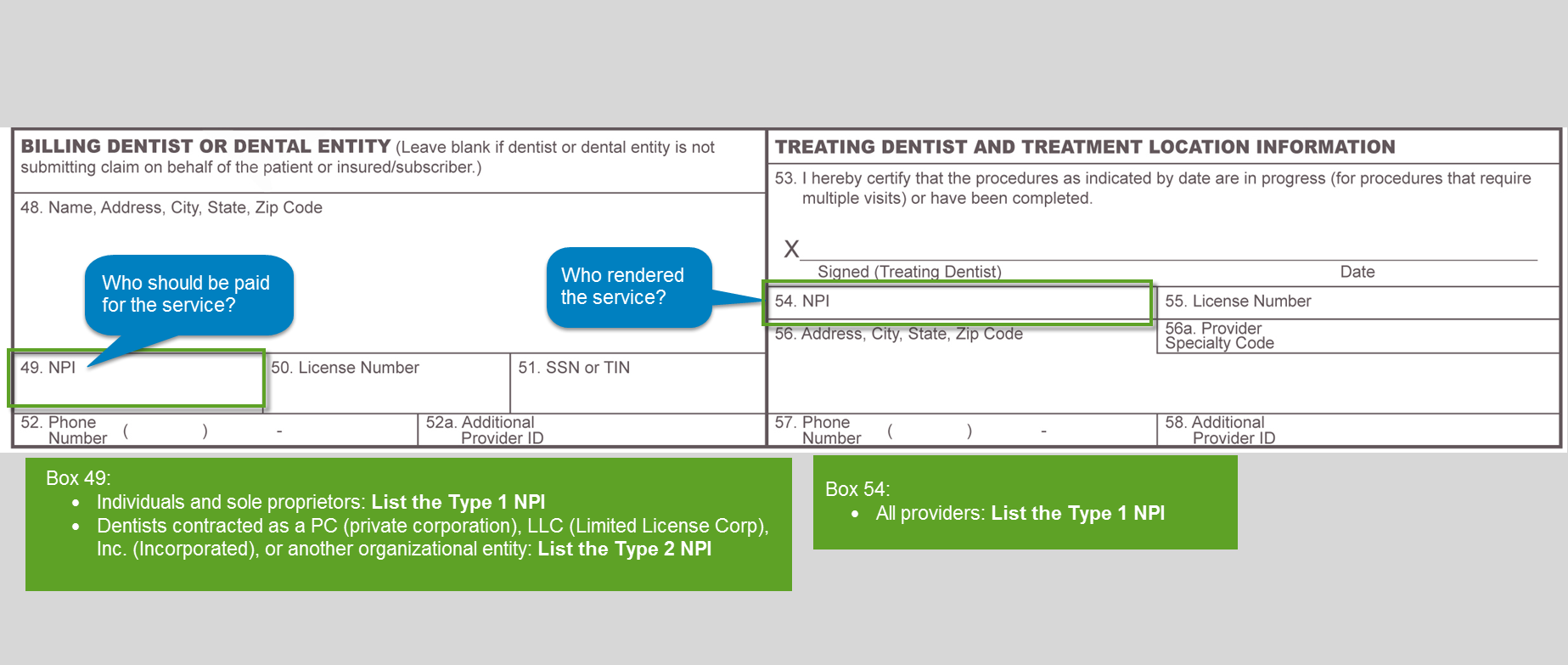
Web How To Fill Out The Ada Dental Claim Form J400Signnowcom On The Web:
Web this pdf editor makes it easy to fill out the ada dental claim form 2019 document. Company/plan name, address, city, state, zip code fold fold policyholder/subscriber information (assigned by. Date of birth (mm/dd/ccyy) 14. The ada dental claim form was revised in 2019 with editorial changes to form captions and check box options for gender (m, f and u) to be consistent with the hipaa standard electronic dental claim (837d).
The Ada Dental Claim Form And The Cdt Manual Are Copyrighted Documents.
Web 2019 ada dental claim form. Type of transaction (mark all applicable boxes) dental claim form statement of actual services epsdt / title 2. Tmhp will continue to accept dental claims submitted on the 2012 and 2018 ada dental claim forms and will update the. Choose the button get form here.
Web The Ada Dental Claim Form Provides A Common Format For Reporting Dental Services To A Patient's Dental Benefit Plan.
Web follow these fast steps to change the pdf printable 2019 ada claim form online for free: I agree to be responsible for all 38. Predetermination/preauthorization number dental benefit plan information 3. I have been informed of the treatment plan and associaled fees.